Introduction
The effect of zoledronic acid, a potent and novel bisphosphonate, on tooth movement and orthodontically induced root resorption in osteoporotic animals systemically treated with zoledronic acid as similarly used in postmenopausal patients has not been elucidated. Therefore, this study was undertaken.
Methods
Fifteen 10-week-old female Wistar rats were divided into 3 groups: ovariectomy, ovariectomy + zoledronic acid, and control. Only the ovariectomy and ovariectomy + zoledronic acid groups underwent ovariectomies. Two weeks after the ovariectomy, zoledronic acid was administered only to the ovariectomy + zoledronic acid group. Four weeks after the ovariectomy, 25-g nickel-titanium closed-coil springs were applied to observe tooth movement and orthodontically induced root resorption.
Results
There were significant differences in the amounts of tooth movement and orthodontically induced root resorption between the ovariectomy and the control groups, and also between the ovariectomy and the ovariectomy + zoledronic acid groups. There was no statistically significant difference in tooth movement and orthodontically induced root resorption between the ovariectomy + zoledronic acid and the control groups. Zoledronic acid inhibited significantly more tooth movement and significantly reduced the severity of orthodontically induced root resorption in the ovariectomized rats. The ovariectomy + zoledronic acid group showed almost the same results as did the control group in both tooth movement and orthodontically induced root resorption.
Conclusions
Zoledronic acid inhibits excessive orthodontic tooth movement and also reduces the risk of severe orthodontically induced root resorption in ovariectomized rats.
Several reviews published over the years have focused on the effects of systemic or local application of several drugs during orthodontic tooth movement. Bisphosphonates have been the most commonly prescribed medications for osteoporotic patients, and their effects on orthodontic tooth movement have been investigated in rat models. Essentially, bisphosphonates are internalized into osteoclasts, leading to inhibition of bone resorption and induction of osteoclast apoptosis.
Zoledronic acid is a potent and novel bisphosphonate that has been recently shown to significantly reduce the risk of fractures in patients who receive the once-yearly dosing regimen for the treatment of postmenopausal osteoporosis. According to several studies, zoledronic acid could be considered the most potent inhibitor of bone resorption compared with other bisphosphonates. Zoledronic acid is a nitrogen-containing, third-generation bisphosphonate with a mechanism of action different from the nonnitrogen-containing bisphosphonates. A recent study has elucidated the pharmacologic properties of third-generation bisphosphonates resulting in the induction of osteoclast apoptosis. Moreover, zoledronic acid has been advocated by several histologic and microcomputed tomography studies showing highly effective prevention of bone loss in ovariectomized rats.
Rat and mouse models have been commonly used for studies of orthodontic tooth movement and orthodontically induced root resorption. Sirisoontorn et al reported that orthodontic tooth movement in ovariectomized rats was more rapid than in the control rats, and orthodontically induced root resorption in ovariectomized rats was more severe than in the control rats. In a recent study, Fujimura et al reported that the local administration of alendronate sodium hydrate inhibited orthodontic tooth movement and root resorption in male mice. Classically, ovariectomized rats have been advocated as a good osteoporotic animal model and often have been used to study the efficacy of drugs aimed to prevent bone loss.
Because of the similarity of the morphology and function of the cells in both root resorption and bone resorption, the processes could be considered similar. In addition, root resorption has been involved not only in osteoclastogenesis but also in odontoclastogenesis via the OPG/RANK/RANKL (osteoprotegerin/receptor activator of nuclear factor kappa B/receptor activator of nuclear factor kappa B ligand) system. Therefore, medications and other substances that have been used to inhibit bone resorption (eg, bisphosphonates) might help to prevent root resorption during orthodontic treatment.
In the last 20 years, the numbers of adult orthodontic patients have dramatically increased. However, studies about pharmaceutics for these patients, especially postmenopausal women, have never completely elucidated their effects because of continually developing drugs and drug regimens.
To date, to our knowledge, no study has reported on the relationship between orthodontic tooth movement and orthodontically induced root resorption in ovariectomized rats with the systemic administration of zoledronic acid. Therefore, the aim of this study was to investigate the effect of zoledronic acid at the same administration as used in postmenopausal patients after orthodontic force application in an osteoporotic rat model.
Material and methods
This study was conducted with approval from the Animal Welfare Committee of Nagasaki University. Some parts of this study were modified after our previous study. Fifteen 10-week-old female Wistar rats (SLC, Shizuoka, Japan; body weight, 170-180 g) were used in this study. The rats were housed in plastic cages in a colony room and fed a standard pellet diet and water ad libitum. After their arrival, the rats were allowed a week for acclimatization before the experiments. The 15 rats were randomly divided into 3 groups of 5 each: ovariectomy and ovariectomy + zoledronic acid experimental groups, and the control group.
Bilateral ovariectomies were performed under general anesthesia by intramuscular injection of ketamine hydrochloride at a dose of 87 mg per kilogram (Ketalar 50; Sankyo, Tokyo, Japan) combined with xylazine hydrochloride at a dose of 13 mg per kilogram (Celactal 2%; Bayer-Japan, Tokyo, Japan). Briefly, the surgical procedure comprised (1) hair removal over the surgical area, (2) a small incision (about 1.0 cm) into the skin halfway between the middle of the back and the base of the tail on both left and right sides, (3) whole ovary removal with a scalpel inserted between the fallopian tubes and the uterine horns, and (4) surgical skin closure. Sham operations were also performed in the control group, in which all procedures were exactly the same, except for the removal of the ovaries. Two weeks after the ovariectomies, zoledronic acid (Zometa; Novartis, Basel, Switzerland) was injected into the peritoneal cavity (1.6 μg/kg) of the ovariectomy + zoledronic acid group and continued once a week for a total of 6 times. The last dose was injected on the same day coinciding with day 21 of the experimental orthodontic tooth movement ( Fig 1 , A ).
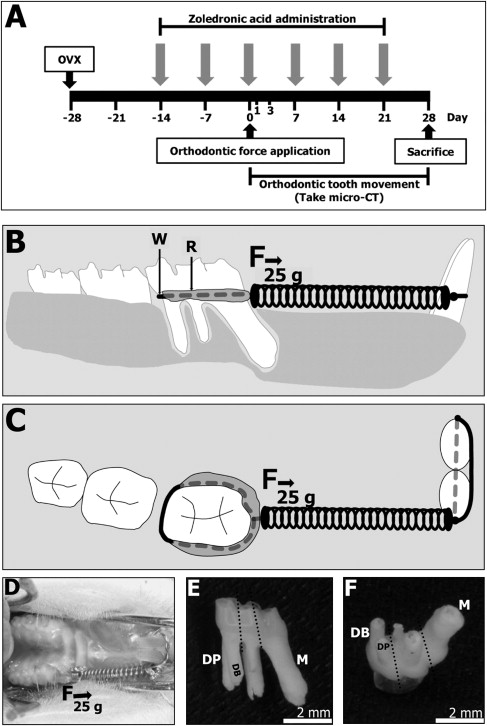
Experimental orthodontic tooth movement was started 4 weeks after the ovariectomies or sham operations. All groups received 25-g nickel-titanium closed-coil springs (Sentalloy; Tomy, Fukushima, Japan) under general anesthesia as previously described to move the maxillary left first molars mesially. The maxillary right first molars with no orthodontic force application served as the negative controls. After the closed-coil springs were set, self-cured resin (Super Bond; Sun Medical, Shiga, Japan) was applied from the distobuccal line angle to the distopalatal line angle on twisted 0.008-in ligature wires that were fixed around the maxillary left first molars ( Fig 1 , B-D ).
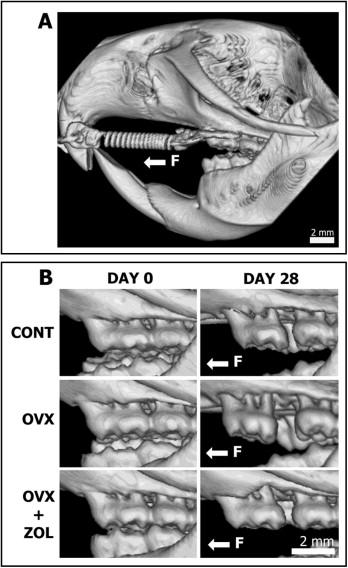
In vivo 3-dimensional (3D) microcomputed tomography (RmCT; Rigaku, Tokyo, Japan) images were taken under general anesthesia as previously described at day 0 (before and immediately after the closed-coil springs were applied) and on days 1, 3, 7, 14, 21, and 28 (before and immediately after the closed-coil springs were removed). At day 28, all rats were killed by carbon dioxide inhalation. Orthodontic tooth movement was measured by 3D image reconstruction software (i-view; J. Morita, Kyoto, Japan) from the microcomputed tomography images of the same rat with the closed-coil spring at days 0 and 28. The distance from the most distal contact point of the maxillary left first molars and the most mesial contact point of the maxillary second molars was calculated as the amount of orthodontic tooth movement in the groups. Furthermore, the microcomputed tomography images from the same rat without the closed-coil spring at days 0 and 28 were used as the representative images from the different groups for superimposition purposes to analyze tooth movement by using 3D medical image analysis software (Ratoc; Ratoc System Engineering, Tokyo, Japan). The same investigator (I.S.) performed all measurements, and every measurement was repeated at 3 separate times. The mean value was used as the final measurement.
After the experimental orthodontic tooth movement was quantified, the rats were killed. The experimental and negative control molars were extracted. All extracted first molars were submerged in 1% sodium hypochlorite for 10 minutes to eliminate the periodontal ligament remnants. The 5 roots of the first molars were divided into 3 parts by using diamond disks ( Fig 1 , E ). Only the mesial and distal roots (distobuccal and distopalatal) were used in this study ( Fig 1 , F ). The mesial surfaces of the roots were scanned with a scanning electron microscope (TM-1000; Hitachi, Tokyo, Japan). The areas of the resorption craters were measured by 3D medical image-processing software (Mimics; Materialise, Leuven, Belgium), and the depths of the root resorption craters were evaluated with a 3D laser scanning microscope (VK-8500; Keyence, Kyoto, Japan) and the image analysis software (Scion Image; Scion, Bethesda, Md). The same investigator (I.S.) performed all measurements, and all measurements were repeated at 3 separate times. The mean value was used as the final measurement.
Statistical analysis
Statistical analysis was performed by using SPSS software (version 16.0; IBM SPSS, Armonk, NY). The Mann-Whitney test was used to compare the amounts of orthodontic tooth movement and orthodontically induced root resorption among the groups.
Results
Experimental orthodontic tooth movement was quantified by using 3D microcomputed tomography images at different experimental days ( Figs 2 and 3 , A ). The amounts of orthodontic tooth movement gradually increased from day 0 until the end of the experiments in all groups. The amount of orthodontic tooth movement in the ovariectomy group was obviously greater than in the ovariectomy + zoledronic acid and the control groups at all time points of the experiment ( Fig 3 , B ; Table I ). Furthermore, the amounts of orthodontic tooth movement in the ovariectomy + zoledronic acid and the control groups showed similar results at all experimental time points ( Figs 2 and 3 ; Table I ). A graph of the orthodontic tooth movement between the ovariectomy + zoledronic acid and the control groups ( Fig 3 , B ) clearly indicates an almost complete overlap with each other during the experiments.
| Rats | Tooth movement (mm) | ||||||
|---|---|---|---|---|---|---|---|
| 0 | 1 | 3 | 7 | 14 | 21 | 28 | |
| Control | |||||||
| 1 | 0.00 | 0.05 | 0.05 | 0.07 | 0.14 | 0.25 | 0.42 |
| 2 | 0.00 | 0.05 | 0.05 | 0.07 | 0.11 | 0.18 | 0.46 |
| 3 | 0.00 | 0.00 | 0.00 | 0.05 | 0.11 | 0.18 | 0.28 |
| 4 | 0.00 | 0.05 | 0.05 | 0.07 | 0.11 | 0.18 | 0.29 |
| 5 | 0.00 | 0.00 | 0.00 | 0.07 | 0.11 | 0.14 | 0.35 |
| Mean | 0.00 | 0.03 | 0.03 | 0.07 | 0.12 | 0.19 | 0.36 |
| SD | 0.00 | 0.03 | 0.03 | 0.01 | 0.01 | 0.04 | 0.08 |
| Median | 0.00 | 0.05 | 0.05 | 0.07 | 0.11 | 0.14 | 0.35 |
| Ovariectomy | |||||||
| 1 | 0.00 | 0.07 | 0.11 | 0.14 | 0.21 | 0.36 | 0.72 |
| 2 | 0.00 | 0.07 | 0.11 | 0.14 | 0.18 | 0.39 | 0.65 |
| 3 | 0.00 | 0.05 | 0.07 | 0.11 | 0.21 | 0.32 | 0.51 |
| 4 | 0.00 | 0.07 | 0.14 | 0.18 | 0.34 | 0.49 | 0.93 |
| 5 | 0.00 | 0.05 | 0.07 | 0.11 | 0.28 | 0.43 | 0.83 |
| Mean | 0.00 | 0.06 | 0.10 | 0.14 | 0.24 | 0.40 | 0.73 |
| SD | 0.00 | 0.01 | 0.03 | 0.03 | 0.07 | 0.07 | 0.16 |
| Median | 0.00 | 0.07 | 0.11 | 0.14 | 0.21 | 0.39 | 0.72 |
| Ovariectomy + zoledronic acid | |||||||
| 1 | 0.00 | 0.00 | 0.00 | 0.05 | 0.11 | 0.14 | 0.22 |
| 2 | 0.00 | 0.00 | 0.00 | 0.05 | 0.11 | 0.15 | 0.25 |
| 3 | 0.00 | 0.05 | 0.05 | 0.07 | 0.11 | 0.18 | 0.36 |
| 4 | 0.00 | 0.05 | 0.05 | 0.07 | 0.14 | 0.18 | 0.36 |
| 5 | 0.00 | 0.05 | 0.05 | 0.07 | 0.14 | 0.18 | 0.42 |
| Mean | 0.00 | 0.03 | 0.03 | 0.06 | 0.12 | 0.17 | 0.32 |
| SD | 0.00 | 0.03 | 0.03 | 0.01 | 0.02 | 0.02 | 0.08 |
| Median | 0.00 | 0.05 | 0.05 | 0.07 | 0.11 | 0.18 | 0.36 |
The superimposition images from the sagittal, axial, and coronal views are shown to represent the amounts and directions of orthodontic tooth movement in all experimental groups. The differences at days 0 and 28 were observed by the overlapped areas of the microcomputed tomography images shown in purple ( Fig 3 , A ). Moreover, the microcomputed tomography images of all experimental groups at day 28 were used to compare the amounts and directions of orthodontic tooth movement. The results of orthodontic tooth movement in the ovariectomy + zoledronic acid group showed almost the same distance as did the control group, evidenced by an almost complete overlap with each other in all sectional views. However, the results of the ovariectomy group were only partially overlapped by the ovariectomy + zoledronic and the control groups in all sectional views ( Fig 3 , A ).
Small amounts of initial orthodontic tooth movement were found in all experimental groups at day 1. These median values were 0.05 mm in the ovariectomy + zoledronic acid and the control groups. The greatest amount of initial orthodontic tooth movement was 0.07 mm in the ovariectomy group ( Fig 3 , B ; Table I ). Dramatic increases of orthodontic tooth movement were found from day 7 until the end of the experiment in all groups, especially in the ovariectomy group ( Fig 3 , B ; Table I ). At day 28, the amounts of orthodontic tooth movement were 0.36 mm in the ovariectomy + zoledronic acid group and 0.35 mm in the control group. The greatest amount of orthodontic tooth movement at day 28 was 0.72 mm in the ovariectomy group. There were significant differences in the distance of orthodontic tooth movement between the ovariectomy and the control groups ( P <0.01 at days 7 and 14; P <0.05 at days 1, 3, 21, and 28) ( Fig 3 , B ; Table I ). In addition, there were significant differences in the distances of orthodontic tooth movement between the ovariectomy and the ovariectomy + zoledronic acid groups ( P <0.05 at days 1, 3, 7, 14, 21, and 28) ( Fig 3 , B ; Table I ). Interestingly, there was no significant difference in the distance of orthodontic tooth movement between the ovariectomy + zoledronic acid and the control groups during the experimental time points ( Fig 3 , B ; Table I ).
The results of orthodontically induced root resorption are shown in the scanning electron microscope images ( Fig 4 ). Three types of orthodontically induced root resorption were clearly identified in all experimental groups: isolated lacunae, wide and shallow resorption pits, and deep resorption craters. Small isolated lacunae were mainly seen on the cervical half of the mesial surfaces on the mesial roots in the ovariectomy + zoledronic acid and the control groups. Wide craters were mainly seen on the distobuccal and distopalatal roots covering the cervical and middle portions of the roots in the ovariectomy +zoledronic and the control groups. In contrast, wide and deep resorption craters were observed in the ovariectomy group scattered on the mesial, distobuccal, and distopalatal roots. These resorption craters were not only at the cervical and middle portions but also at the apical portions of the roots.
The results of orthodontically induced root resorption in the ovariectomy group showed more severe root resorption than in the ovariectomy + zoledronic acid and the control groups in areas, depths, and volumes ( Table II ) quantified on the mesial, distobuccal, and distopalatal roots. Furthermore, the results of the total volume of root resorption in the 3 roots in the ovariectomy group showed larger root resorption craters than those in the ovariectomy + zoledronic acid and the control groups ( Fig 5 ; Table III ). Almost the same severity of orthodontically induced root resorption was found between the ovariectomy + zoledronic acid and the control groups in all parameters—area, depth, and volume ( Table II ) investigated on the mesial, distobuccal, and distopalatal roots. Moreover, the results of the total volumes in the 3 roots of the ovariectomy + zoledronic acid group showed almost the same severity as in the control group ( Fig 5 ; Table III ). There were significant differences ( P <0.05) in area, depth, and volume of orthodontically induced root resorption between the ovariectomy and the control groups analyzed in the mesial, distobuccal, and distopalatal roots and also in the total volume of orthodontically induced root resorption in the 3 roots ( Fig 5 ). Similarly, there were significant differences ( P <0.05) in the severity of orthodontically induced root resorption between the ovariectomy and the ovariectomy + zoledronic acid groups in area, depth, and volume identified on the mesial, distobuccal, and distopalatal roots and also the total volume of orthodontically induced root resorption in the 3 roots ( Fig 5 ). However, there was no significant difference in the severity of orthodontically induced root resorption between the ovariectomy + zoledronic acid and the control groups in area, depth, and volume on the mesial, distobuccal, and distopalatal roots and also the total volume of orthodontically induced root resorption in the 3 roots ( Fig 5 ).
| Mesial | Distobuccal | Distopalatal | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | Ovariectomy | Ovariectomy + zoledronic acid |
Control | Ovariectomy | Ovariectomy + zoledronic acid |
Control | Ovariectomy | Ovariectomy + zoledronic acid |
|
| Area of orthodontically induced root resorption (× 10 2 μm 2 ) | |||||||||
| 1 | 11.37 | 23.82 | 3.18 | 11.44 | 33.87 | 5.16 | 16.99 | 33.49 | 2.49 |
| 2 | 12.51 | 21.89 | 18.53 | 13.85 | 35.52 | 12.75 | 14.28 | 35.12 | 17.73 |
| 3 | 14.81 | 23.31 | 5.29 | 7.75 | 30.99 | 13.43 | 15.45 | 28.98 | 18.47 |
| 4 | 4.51 | 18.84 | 11.24 | 11.51 | 40.04 | 3.23 | 19.52 | 39.19 | 5.20 |
| 5 | 4.29 | 18.75 | 4.26 | 3.41 | 32.36 | 4.66 | 9.95 | 26.52 | 7.15 |
| Mean | 9.50 | 21.32 | 8.50 | 9.59 | 34.56 | 7.85 | 15.24 | 32.66 | 10.21 |
| SD | 4.82 | 2.41 | 6.42 | 4.09 | 3.50 | 4.85 | 3.55 | 5.02 | 7.40 |
| Median | 11.37 | 21.89 | 11.24 | 11.44 | 33.87 | 11.27 | 15.45 | 33.49 | 15.28 |
| Depth of orthodontically induced root resorption (μm) | |||||||||
| 1 | 7.37 | 40.24 | 4.98 | 18.50 | 56.82 | 16.40 | 16.89 | 45.43 | 10.05 |
| 2 | 4.12 | 13.20 | 4.96 | 9.11 | 54.93 | 13.90 | 12.71 | 44.45 | 13.51 |
| 3 | 6.28 | 32.94 | 5.75 | 11.55 | 46.69 | 16.89 | 14.99 | 41.70 | 17.16 |
| 4 | 6.98 | 37.09 | 5.73 | 18.50 | 39.32 | 11.38 | 16.89 | 36.82 | 12.95 |
| 5 | 4.13 | 37.79 | 7.20 | 9.30 | 37.41 | 10.11 | 16.97 | 36.05 | 12.39 |
| Mean | 5.78 | 32.25 | 5.72 | 13.39 | 47.03 | 13.74 | 15.69 | 40.89 | 13.21 |
| SD | 1.56 | 10.97 | 0.91 | 4.76 | 8.81 | 2.99 | 1.86 | 4.30 | 2.57 |
| Median | 6.28 | 37.09 | 5.73 | 11.55 | 46.69 | 13.90 | 16.89 | 41.70 | 12.95 |
| Volume of orthodontically induced root resorption (10 4 μm 3 ) | |||||||||
| 1 | 0.84 | 9.59 | 0.16 | 2.12 | 19.24 | 0.85 | 2.87 | 15.21 | 0.25 |
| 2 | 0.52 | 2.89 | 0.92 | 1.26 | 19.51 | 1.77 | 1.81 | 15.61 | 2.40 |
| 3 | 0.93 | 7.68 | 0.30 | 0.90 | 14.47 | 2.27 | 2.32 | 12.08 | 3.17 |
| 4 | 0.31 | 6.99 | 0.64 | 2.13 | 15.74 | 0.37 | 3.30 | 14.43 | 0.67 |
| 5 | 0.18 | 7.09 | 0.31 | 0.32 | 12.11 | 0.47 | 1.69 | 9.56 | 0.89 |
| Mean | 0.56 | 6.85 | 0.47 | 1.34 | 16.21 | 1.15 | 2.40 | 13.38 | 1.47 |
| SD | 0.33 | 2.45 | 0.31 | 0.79 | 3.17 | 0.84 | 0.69 | 2.54 | 1.25 |
| Median | 0.52 | 7.09 | 0.31 | 1.26 | 15.74 | 0.85 | 2.32 | 12.08 | 0.89 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


