Establishment of a treatment plan is based on efficacy and easy application by the clinician, and acceptance by the patient. Treatment of adult patients with Class III malocclusion might require orthognathic surgery, especially when the deformity is severe, with a significant impact on facial esthetics. Impacted teeth can remarkably influence treatment planning, which should be precise and concise to allow a reasonably short treatment time with low biologic cost. We report here the case of a 20-year-old man who had a skeletal Class III malocclusion and impaction of the maxillary right canine, leading to remarkable deviation of the maxillary midline; this was his chief complaint. Because of the severely deviated position of the impacted canine, treatment included extraction of the maxillary right canine and left first premolar for midline correction followed by leveling, alignment, correction of compensatory tooth positioning, and orthognathic surgery to correct the skeletal Class III malocclusion because of the severe maxillary deficiency. This treatment approach allowed correction of the maxillary dental midline discrepancy to the midsagittal plane and establishment of good occlusion and optimal esthetics.
Among the hard-tissue structures involved in Class III malocclusions, there are some variations such as mandibular prognathism, maxillary retrusion, or a combination of both. Maxillary deficiency is more frequent, accounting for 60% to 63% of Class III malocclusions. Thus, for a correct diagnosis and a good prognosis, it is essential to identify the deformity and its primary etiologic agent. The skeletal deficiency at the maxillary region can also be associated with deficiency of the facial middle third, confirmed by the contour of the malar bone, orbital ridge, and subpupillary area, which can be described as flattened, soft, normal (convex), or prominent. Intraoral examination shows excessive buccal inclination of the maxillary incisors and lingual inclination of the mandibular incisors, in an attempt to mask the real maxillomandibular discrepancy. The basal bone deficiency is reflected in the facial soft tissues, causing an unfavorable esthetic impact that can affect the patient’s self-esteem. The literature reports that a Class III malocclusion caused by maxillary deficiency should be treated as early as possible because it has an immediate positive esthetic impact and can redirect this unfavorable maxillary growth. The protocol most often used at this stage is rapid maxillary expansion followed by maxillary protraction. However, because of the high rate of relapse of Class III malocclusions, patients having early treatment should be carefully followed until their growth is completed. On the other hand, if a young patient obtains treatment at an early age, his or her skeletal discrepancy worsens with facial growth. Therefore, if the patient’s chief complaint is facial esthetics, a combined orthodontic-surgical approach could satisfy the need. Our aim in this case report was to discuss this treatment approach and its pros and cons.
Diagnosis and etiology
A young man, 20 years old, sought orthodontic treatment at a private practice in Bauru, São Paulo, Brazil, with the chief complaints of maxillary dental midline deviation to the right of the midsagittal plane, clinical absence of the maxillary right canine, and unfavorable facial appearance.
Frontal analysis showed a constantly tired-looking face, passive lip competence with poor volume, inadequate lip vermilion especially at the upper lip, and an evident maxillary midline deviation to the right on smiling ( Figs 1 and 2 ). The profile analysis showed a Class III aspect consequent to maxillary and zygomatic deficiencies; however, the chin-neck line was good, and the chin appearance was satisfactory.
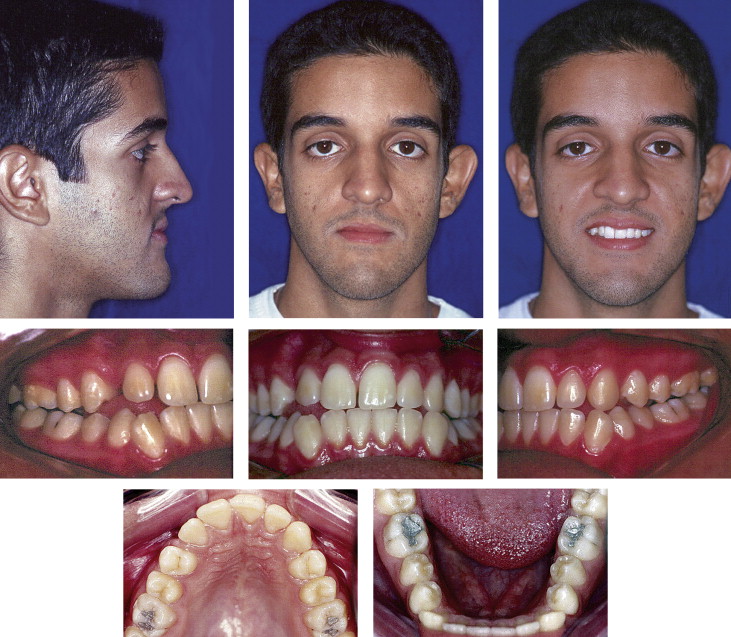
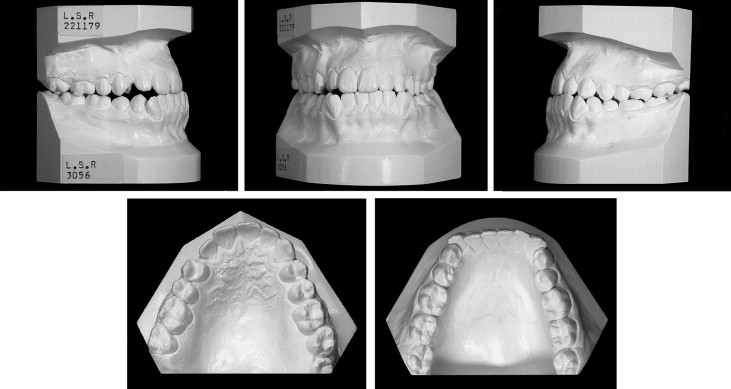
The occlusal examination showed a narrow maxilla, Class III molar relationships on both sides, spacing between the maxillary right lateral incisor and first premolar, clinical absence of the maxillary right canine, and an edge-to-edge incisor relationship in centric relation ( Figs 1 and 2 ).
The maxillary right canine was high in the palate, mesially displaced, and above the central and right lateral incisors. Additionally, the maxillary right third molar was missing ( Figs 3 and 4 ). Cephalometrically, the maxillomandibular relationship was deficient, with an accentuated mandibular protrusion that contradicted the clinical facial evaluation ( Fig 4 , Table I and Table II ). Overall, there was an equilibrated growth pattern, with slight discrepancies among some variables. The maxillary and mandibular incisors were slightly retruded and lingually tipped. Overjet and overbite were reduced, and there was a Class III molar relationship. The concave soft-tissue profile accentuated the underlying skeletal discrepancies with the retrusion of the upper and lower lips ( Table II ).


| Maxillary component | |
| A-Nperp | Distance from A-point to nasion-perpendicular, allows evaluation of the maxilla in the sagittal direction. |
| Co-A | Distance from condylion to A-point. |
| Palatal plane-Frankfort plane | Angle formed between the palatal plane and Frankfort plane. |
| Mandibular component | |
| Pg-Nperp | Distance between pogonion and nasion-perpendicular, allows evaluation of the mandible in the sagittal direction. |
| Co-Gn | Distance from condylion to gnathion. |
| Maxillomandibular relationship | |
| NAP | Degree of convexity of the bony profile. |
| Wits appraisal | Maxillomandibular relationship, measured from points A to B, perpendicular to the functional occlusal plane. |
| Growth pattern | |
| SnGoGn | Angle between the SN line and the mandibular plane, indicates the relationship between the mandible and the anterior skull base in the vertical direction. |
| Facial axis angle | Angle between the basion-nasion plane and the facial axis, indicates chin position and growth, and the relationship between facial height and depth. |
| FMA | Frankfort-mandibular plane angle. |
| Maxillary and mandibular dentoalveolar components | |
| 1.NA | Maxillary incisor long axis to NA angle. |
| 1-NA | Distance between the most anterior point of the crown of the maxillary incisor and NA line. |
| 1-APerp | Distance between the most anterior point of the maxillary central incisor crown and anterior nasal spine perpendicular. Values posterior to this line were considered negative; values anterior to it were regarded as positive. |
| 1.NB | Mandibular incisor long axis to NB angle. |
| 1-NB | Distance between the most anterior point of the crown of the mandibular incisor and the NB line. |
| 1-A-Pog | Distance between the most anterior point of the mandibular central incisor crown and pogonion perpendicular. It determines the sagittal position of the mandibular central incisor in relation to the mandible and its increase indicates incisor protrusion. |
| IMPA | Angle between the mandibular plane and long axis of the mandibular incisor, indicates the degree of inclination of the mandibular incisor. |
| Dental relationships | |
| 1.1 | Angle between the maxillary and mandibular incisors’ long axes. |
| Overbite | Distance from the incisal edge of the mandibular incisor to the incisal edge of the maxillary incisor, measured perpendicular to the functional occlusal plane. |
| Overjet | Distance from the incisal edge of the mandibular incisor to the incisal edge of the maxillary incisor, measured parallel to the functional occlusal plane. |
| Molar relationship | Horizontal distance of the perpendicular projections of the maxillary and mandibular first molars’ mesial surfaces on the functional occlusal plane. Positive values were attributed when the mandibular molars were mesial to the maxillary molars. |
| Occlusal plane-ramus Xi | Distance between the occlusal plane and the center of the ramus (Xi point). |
| Soft tissue | |
| H-NB | Angle formed by the Holdaway esthetic and NB lines, indicates the degree of convexity of the soft-tissue profile. |
| Upper lip-line S | Distance from S line to the most anterior point of the upper lip. |
| Lower lip-line S | Distance from S line to the most anterior point of the lower lip. |
| Nasolabial angle | Angle between the lower nasal margin and the tangent to the upper lip, originating at subnasale. It allows evaluation of protrusion of the upper lip in relation to the lower nasal margin. |
| Upper lip protrusion-esthetic line | Distance from the Ricketts’ esthetic line to upper lip protrusion. |
| Lower lip protrusion-esthetic line | Distance from the Ricketts’ esthetic line to lower lip protrusion. |
| Mentolabial sulcus | Deepest point in the mentolabial sulcus perpendicular to the line through the most prominent point on the lower lip and soft-tissue chin. |
| Initial (July 7, 1999) |
Presurgical (December 3, 2002) |
Final (October 4, 2004) |
|
|---|---|---|---|
| Maxillary component | |||
| A-Nperp (mm) | 2.9 | 0.9 | 2.9 |
| SNA (°) | 78.3 | 77.2 | 79.4 |
| Co-A (mm) | 94.2 | 95.7 | 96.9 |
| Palatal plane-Frankfort plane (°) | –3.9 | –4.9 | –9.0 |
| Mandibular component | |||
| Pg-Nperp (mm) | 10.3 | 6.1 | 6.4 |
| SNB (°) | 77.6 | 76.2 | 76.4 |
| Co-Gn (°) | 132.8 | 132.8 | 134.2 |
| Maxillomandibular relationships | |||
| Maxillomandibular difference (°) | 38.6 | 37.1 | 37.3 |
| NAP (°) | –4.0 | –3.9 | –0.1 |
| ANB (°) | 0.6 | 0.9 | 3.0 |
| Wits appraisal (mm) | –1.5 | –0.4 | 1.4 |
| Growth pattern | |||
| Facial axis angle (°) | 5.1 | 5.5 | 4.6 |
| SN.GoGn (°) | 38.8 | 38.6 | 38.2 |
| SN.Gn (°) | 68.7 | 69.2 | 69.5 |
| FMA (°) | 24.8 | 25.0 | 24.7 |
| Maxillary dentoalveolar component | |||
| 1.NA (°) | 21.3 | 26.4 | 22.3 |
| 1-NA (mm) | 2.2 | 0.6 | 3.9 |
| 1-APerp (mm) | 3.5 | 1.0 | 5.5 |
| Mandibular dentoalveolar component | |||
| 1.NB (°) | 17.4 | 36.1 | 31.7 |
| 1-NB (mm) | 1.5 | 7.8 | 5.9 |
| 1-APog (mm) | –1.2 | 4.5 | 1.3 |
| P-NB (mm) | 5.5 | 6.3 | 6.5 |
| IMPA (°) | 80.7 | 101.2 | 97.0 |
| Dental relationships | |||
| 1.1 (°) | 140.7 | 116.6 | 123.0 |
| Overbite (mm) | 0.3 | 0.6 | 1.7 |
| Overjet (mm) | 1.6 | –5.7 | 2.6 |
| Molar relationship (mm) | –6.0 | –1.4 | 2.7 |
| Occlusal plane-ramus Xi (mm) | 0.2 | 2.0 | 1.9 |
| Soft tissues | |||
| H.NB (°) | –4.7 | –8.2 | –0.7 |
| H-nose (mm) | 19.2 | 22.8 | 16.0 |
| Upper lip-S (mm) | –10.0 | –11.4 | –7.1 |
| Lower lip-S (mm) | –6.4 | –3.5 | –6.0 |
| Nasolabial angle (°) | 102.2 | 108.1 | 96.4 |
| Upper lip protrusion-esthetic plane (mm) | –1.9 | –3.2 | 0.7 |
| Lower lip protrusion-esthetic plane (mm) | –1.2 | 1.8 | –0.8 |
| Mentolabial sulcus (mm) | 4.1 | 5.7 | 6.4 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


