This case report describes the orthodontic treatment with autotransplantation and bone grafting of the lost maxillary alveolus for a patient injured in a traffic accident. This patient had a severe skeletal Class III relationship because of the loss of 6 maxillary teeth and the adjacent alveolar bone. Autotransplantation of mandibular first premolars and bone grafting of the deficient alveolus were carried out to improve the occlusion and the profile. After orthodontic treatment, the transplanted premolars were reshaped and restored with composite as central incisors. Good occlusion and cosmetic improvement were obtained. Orthodontic treatment is useful for occlusal reconstruction after a traumatic injury, and autotransplantation is an effective option for these patients.
Traumatic maxillofacial fractures can sometimes cause life-threatening neurologic injuries. Therefore, emergency treatment for these patients is critical, and they are typically brought to a hospital emergency room, where a general surgeon performs surgery without concern for the occlusion. If fractured alveolar bone and displaced teeth are removed during the emergency surgery, subsequent occlusal reconstruction can be quite difficult.
Autotransplantation has been reported as a treatment for anterior tooth loss. Due to the unique osteogenic capacity of an autotransplanted tooth, this procedure is a unique treatment alternative when both the lost teeth and the atrophic or missing alveolar process must be replaced. We report here on a patient who lost her anterior maxilla and 6 maxillary anterior teeth in an accident. The treatment involved bone grafting, autotransplantation, orthodontic treatment, and restoration.
Diagnosis and etiology
The patient was a 10-year-old girl who had been hit by a truck while riding her bicycle. She was transported to the hospital in an ambulance. She was bruised on her face and lips, and her maxillary anterior alveolar bone and the 6 anterior teeth were lost because of the fracture. After recovering from her injuries, she visited a general dentist because of her parents’ concerns regarding her cosmetic appearance and her difficulty in masticating food. She was referred to the clinic for adjunctive orthodontic treatment to help in her rehabilitation.
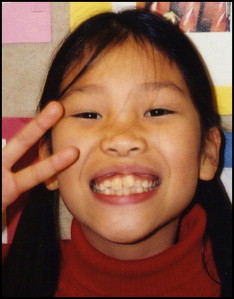
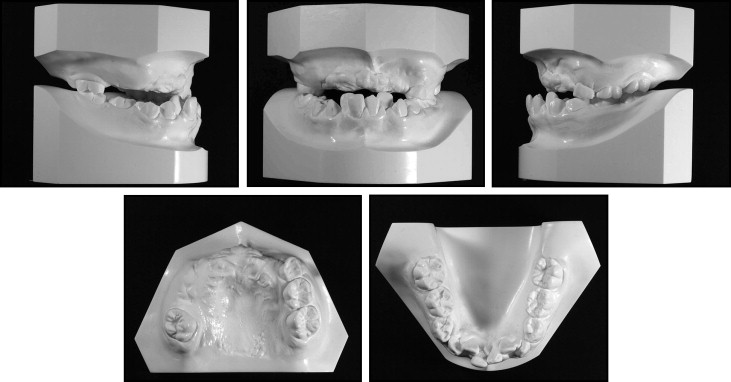
At her initial visit, 1 month after the injury, she had only 2 permanent first molars and her left first and second deciduous molars in the maxilla ( Figs 1-5 ). The mandibular anterior teeth were crowded and extruded with an excessive curve of Spee. Her molar relationship was Class I. The crowns of both mandibular central incisors had also been fractured in the accident but had no pulp exposure, so the right central incisor had been restored with composite by her general dentist. Her facial profile showed severe prognathism with a retropositioned midface that resembled an elderly person and was exaggerated by the missing maxillary anterior teeth. However, her facial photograph before the traffic accident showed excessive overjet of her rotated anterior teeth, and a slight Class III tendency with a prominent chin ( Fig 2 ). No other significant damage to the cranium and face was observed on the 3-dimensional computed tomography image ( Fig 4 , A ), and there were no other fractures of the maxilla ( Fig 4 , B ).

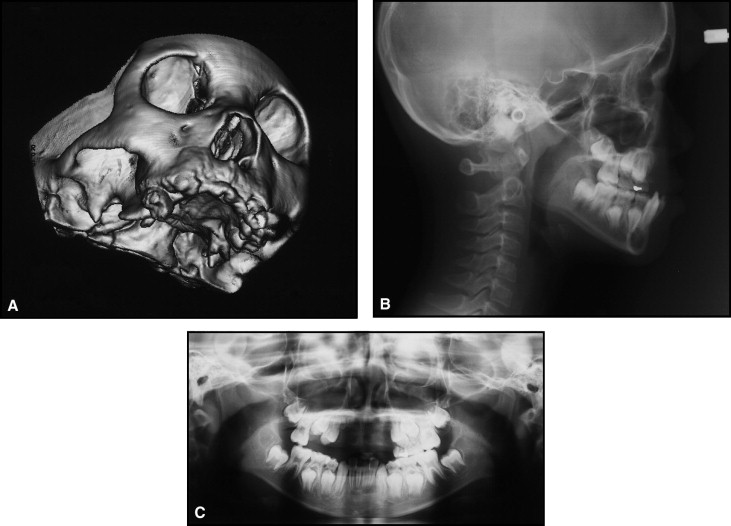
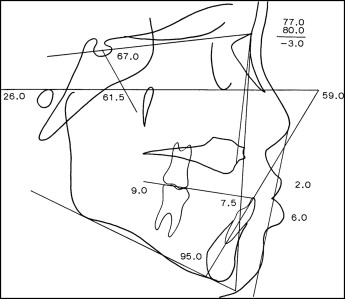
The cephalometric analysis showed a skeletal Class III relationship (ANB, −3.0°) with an extremely retruded maxilla (SNA, 77.0°) because of the loss of the anterior alveolar segment, and a slightly protruded mandible (SNB, 80.0°). The mandibular incisors were inclined labially (IMPA, 95°; FMIA, 59.0°; L1-APo, 7.5 mm) ( Fig 5 , Table ). The absence of the maxillary anterior teeth had caused a tongue-thrusting habit. The panoramic radiograph showed 8 permanent teeth in the maxilla and 14 in the mandible in addition to the developing third molars ( Fig 4 , C ).
| Measurement | Standard | Initial | Final |
|---|---|---|---|
| SNA angle (°) | 82.3 | 77 | 77 |
| SNB angle (°) | 78.9 | 80 | 75 |
| ANB angle (°) | 3.4 | −3 | 2 |
| MP to FH (°) | 28.8 | 26 | 26 |
| Y-axis (°) | 65.4 | 61.5 | 64 |
| FMIA (°) | 54.9 | 59 | 60 |
| L1 to MP (°) | 96.3 | 95 | 94 |
| L1 to APo (mm) | 3 | 7.5 | 1 |
| U1 to FH (°) | 111.1 | Unmeasurable | 115 |
| U1 to SN (°) | 104.5 | Unmeasurable | 109.5 |
| Interincisal angle (°) | 124.1 | Unmeasurable | 125 |
Treatment objectives and plan
Planning treatment for a young patient who has lost so many teeth and alveolar bone involves a detailed evaluation of both the prognosis for the injured teeth and the prosthodontic treatment plan. A coordinated approach, incorporating clinical and radiographic findings of the healing and potential complications, must be established before orthodontic treatment can start. The plan should be based on a realistic evaluation of the prognosis for the injured teeth, the future prosthodontic treatment, and the orthodontic difficulties.
Our patient’s chronologic age was 10, so subsequent mandibular forward growth would worsen the jaw relationship. Labial proclination of her mandibular incisors was also expected because of the tongue-thrusting habit. Therefore, chincup therapy was indispensable to inhibit mandibular advancement and to upright the mandibular incisors.
There were 6 fewer teeth in the maxillary arch, and the mandibular incisors were labially inclined and crowded, so extraction of the mandibular first premolars was planned. Even with mandibular extractions, there were 4 more maxillary teeth compared with the number of mandibular teeth. However, if the extracted mandibular premolars could be transplanted to the maxilla, the difference in the numbers of teeth in the jaws would decrease to 2. After orthodontic treatment, the 2 missing incisors could be replaced by dental implants. When 2 implants are placed side by side, it is usually not possible to create a satisfactory gingival papilla between the implants. So we decided to place the transplanted premolars into the maxillary central incisor positions.
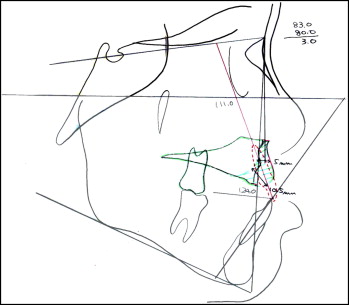
Because of the associated bone loss, bone grafting was necessary to obtain a normal interincisal relationship and to enhance midface advancement. The amount of bone grafting to the anterior maxilla was estimated by cephalometric prediction ( Fig 6 ). The amount of the bone graft and the tooth inclination were estimated without retraction of the mandibular incisors, because the mandible could grow forward and worsen the ANB angle.
The panoramic radiograph showed that the root formation of both premolars was incomplete, and the apices were open. The success of autotransplantation and the ability to maintain tooth vitality of the donor teeth are enhanced if the transplantation occurs before the completion of root formation.
The crown forms of the transplanted premolars would require reshaping with composite after orthodontic treatment. Two single-tooth implants would eventually be placed in the maxilla to replace the lateral incisors after the patient had completed her facial growth.
Treatment objectives and plan
Planning treatment for a young patient who has lost so many teeth and alveolar bone involves a detailed evaluation of both the prognosis for the injured teeth and the prosthodontic treatment plan. A coordinated approach, incorporating clinical and radiographic findings of the healing and potential complications, must be established before orthodontic treatment can start. The plan should be based on a realistic evaluation of the prognosis for the injured teeth, the future prosthodontic treatment, and the orthodontic difficulties.
Our patient’s chronologic age was 10, so subsequent mandibular forward growth would worsen the jaw relationship. Labial proclination of her mandibular incisors was also expected because of the tongue-thrusting habit. Therefore, chincup therapy was indispensable to inhibit mandibular advancement and to upright the mandibular incisors.
There were 6 fewer teeth in the maxillary arch, and the mandibular incisors were labially inclined and crowded, so extraction of the mandibular first premolars was planned. Even with mandibular extractions, there were 4 more maxillary teeth compared with the number of mandibular teeth. However, if the extracted mandibular premolars could be transplanted to the maxilla, the difference in the numbers of teeth in the jaws would decrease to 2. After orthodontic treatment, the 2 missing incisors could be replaced by dental implants. When 2 implants are placed side by side, it is usually not possible to create a satisfactory gingival papilla between the implants. So we decided to place the transplanted premolars into the maxillary central incisor positions.
Because of the associated bone loss, bone grafting was necessary to obtain a normal interincisal relationship and to enhance midface advancement. The amount of bone grafting to the anterior maxilla was estimated by cephalometric prediction ( Fig 6 ). The amount of the bone graft and the tooth inclination were estimated without retraction of the mandibular incisors, because the mandible could grow forward and worsen the ANB angle.


