Armamentarium
| Traditional Open Technique |
|
| Endoscopic-Assisted Technique |
|
History of the Procedure
The surgical management of orbital fractures continues to be a challenging field because no single approach or reconstruction material is suitable for all patients. In addition, the technical demands of the surgical repair and the related anatomy make precise repair difficult for the novice. The surgeon must ensure gentle tissue handling and careful globe retraction to allow for visualization of the fracture during operative repair.
Signs and symptoms of orbital fractures have been described throughout recorded human history. In 1957, Smith and Regan coined the term orbital blow-out fracture after they reproduced orbital floor and medial wall fractures in cadavers by hammering a hurling ball resting on the eye. In 1960, Converse and Smith classified these fractures as “pure” (isolated floor) and “impure” (floor and rim). A year later, Converse et al discussed reconstruction of orbital floor fractures by coordinating graft volume replacement with orbital volume increase to avoid enophthalmos. In 1986, Manson et al suggested that the shape and position of the orbital graft/implant are more important than the orbital volume; they emphasized that the bony floor anatomy (bulge in the orbital floor) is instrumental in providing support to the globe.
More recently, several technologic advances have affected the surgical management of orbital fractures, such as virtual planning surgery, custom-made implants, navigation, and intraoperative computed tomography (CT) scanning. The traditional technique uses either periorbital incisions or overlying lacerations. Orbital roof fractures may be directly accessed and repaired using a frontal craniotomy and brain retraction.
The initial use of endoscopic techniques in the diagnosis and management of orbital fractures can be traced to the 1970s, when Westphal and Kreidler described sinusoscopy for the diagnosis of blow-out fractures. However, the development of fine-cut CT scans for evaluation of these fractures obviated the need for this procedure in the ensuing years. In 1997, Saunders et al described the transantral approach for repair of orbital floor fractures, and in 1999, Chen et al described the endonasal approach for repair of medial wall fractures. A primary advantage of endoscopic repair is the avoidance of periorbital incisions, which may contribute to an unesthetic postoperative appearance and lid function problems.
History of the Procedure
The surgical management of orbital fractures continues to be a challenging field because no single approach or reconstruction material is suitable for all patients. In addition, the technical demands of the surgical repair and the related anatomy make precise repair difficult for the novice. The surgeon must ensure gentle tissue handling and careful globe retraction to allow for visualization of the fracture during operative repair.
Signs and symptoms of orbital fractures have been described throughout recorded human history. In 1957, Smith and Regan coined the term orbital blow-out fracture after they reproduced orbital floor and medial wall fractures in cadavers by hammering a hurling ball resting on the eye. In 1960, Converse and Smith classified these fractures as “pure” (isolated floor) and “impure” (floor and rim). A year later, Converse et al discussed reconstruction of orbital floor fractures by coordinating graft volume replacement with orbital volume increase to avoid enophthalmos. In 1986, Manson et al suggested that the shape and position of the orbital graft/implant are more important than the orbital volume; they emphasized that the bony floor anatomy (bulge in the orbital floor) is instrumental in providing support to the globe.
More recently, several technologic advances have affected the surgical management of orbital fractures, such as virtual planning surgery, custom-made implants, navigation, and intraoperative computed tomography (CT) scanning. The traditional technique uses either periorbital incisions or overlying lacerations. Orbital roof fractures may be directly accessed and repaired using a frontal craniotomy and brain retraction.
The initial use of endoscopic techniques in the diagnosis and management of orbital fractures can be traced to the 1970s, when Westphal and Kreidler described sinusoscopy for the diagnosis of blow-out fractures. However, the development of fine-cut CT scans for evaluation of these fractures obviated the need for this procedure in the ensuing years. In 1997, Saunders et al described the transantral approach for repair of orbital floor fractures, and in 1999, Chen et al described the endonasal approach for repair of medial wall fractures. A primary advantage of endoscopic repair is the avoidance of periorbital incisions, which may contribute to an unesthetic postoperative appearance and lid function problems.
Indications for the Use of the Procedure
Orbital fractures can be encountered in a number of clinical presentations, such as naso-orbito-ethmoid (NOE) fractures, orbitozygomaticomaxillary complex fractures, and internal orbital fractures. The discussion in this chapter focuses on the surgical management of isolated internal orbital fractures; other types of fractures are described elsewhere in this text.
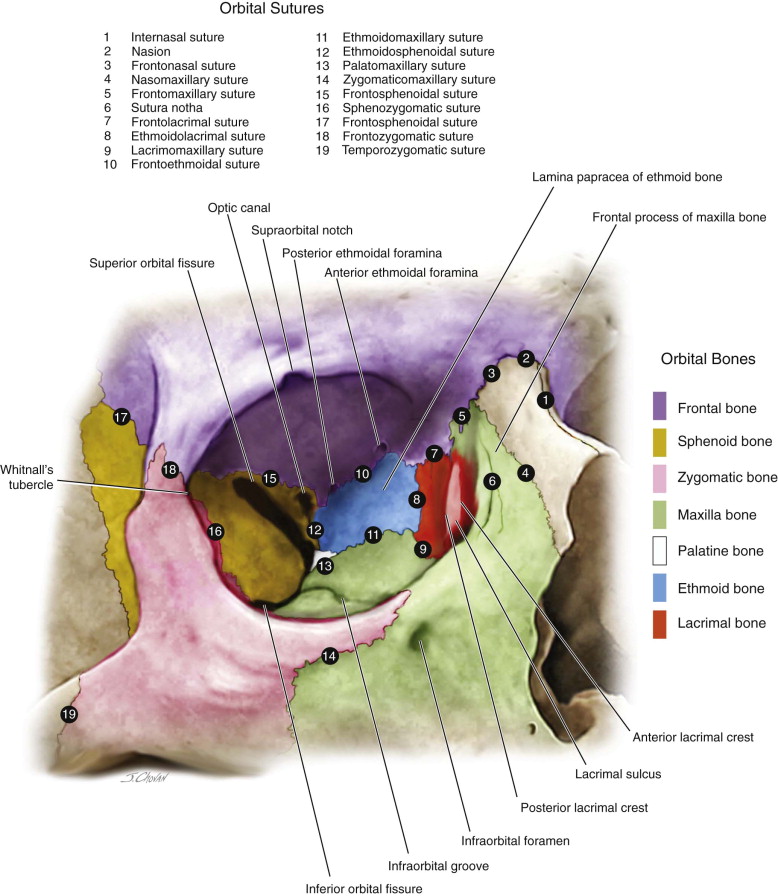
The bony orbit supports and protects the globe and allows for functioning of the eye. It is shaped like a pyramid, with the base making up the orbital rim. Seven bones form the orbit. The frontal bone and lesser wing of the sphenoid make up the orbital roof. The floor of the orbit is composed of the orbital portions of the maxillary and zygomatic bones. On the medial aspect of the orbit lies the lamina papyracea of the ethmoid, the frontal process of the maxilla, and the lacrimal and sphenoid bones. The lesser wing of the sphenoid and zygoma form the lateral wall. Any or all of these bones can be involved in orbital blow-out fractures; however, usually either the floor or the medial wall is involved because these are the thinnest components ( Figure 74-1 ). Blow-in fractures are possible and most likely involve the orbital roof. Although outside the scope of this chapter, blow-in fractures of the orbital roof require special attention. They not only increase orbital volume and therefore are compressive on the orbital space, they also can involve herniation of the brain into the orbital space, with a characteristic pulsation felt by the patient. Neurosurgical consultation is warranted for these fractures.
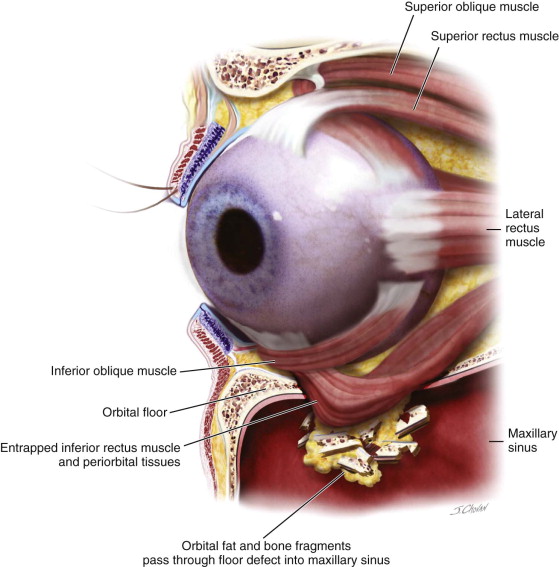
Regardless of the clinical presentation, indications for surgery are divided into functional or esthetic reasons. Functional indications for surgery are related to either impingement by the fracture on the surrounding soft tissues or defects from fractures that are large enough to cause significant hypoglobus, resulting in visual changes. An ophthalmologist skilled in trauma care should evaluate all patients with orbital fractures, especially those with acute visual changes. Soft tissue structures that maybe impinged upon or injured by the fracture can include the optic nerve, blood vessels, the second division of the trigeminal nerve, the motor nerves to the globe, muscles, and the periorbita itself. Although fortunately rare, both orbital apex syndrome and superior orbital fissure syndrome also can occur. Most functional issues are related to entrapment of the periorbita or rectus muscles by the fracture ( Figure 74-2 ). This may cause restriction of gaze, with resultant diplopia in the affected visual field. This can be clinically confirmed with a forced duction test of the affected muscle.
In most circumstances, orbital fractures with functional indications for repair should be considered urgent cases. Esthetic indications for repair are mostly due to globe malposition. In these cases, enophthalmos and hypoglobus are commonly encountered. The severity of these signs and symptoms dictate the need for either an observational period or early surgical repair. Occasionally, patients present with a large defect but are free of signs and symptoms. In these cases, surgery should still be considered because studies have shown a correlation between globe position and the size and location of the defect. Most facial trauma surgeons agree that a 2 × 2 cm fracture defect behind the equator of the globe most likely will cause clinically significant enophthalmos (greater than 2 mm), and these patients are candidates for surgical repair. Special consideration should be given to orbital fractures in children with clinical or radiographic evidence of entrapment (also termed a “white-eyed blowout”). Clinically, these patients demonstrate entrapment and may also present with the ocular-cardiac reflex, which may cause significant bradycardia, heart block, and nausea and vomiting. The bony elasticity of the facial skeleton in children allows the orbital fracture to open and close back into position, tightly trapping periorbital soft tissues or muscles. Within 24 hours, involved muscle tissue may undergo avascular necrosis, with a resultant Volkmann ischemic contracture. This causes permanent muscle imbalance and results in lifelong diplopia unless corrected surgically. Orbital entrapment in children is regarded as a surgical emergency and should be repaired immediately ( Figure 74-3 ).


Although the indications for endoscopic techniques are similar to those for the traditional approach, not all orbital fractures can be repaired endoscopically. In the authors’ experience, small to medium-sized central orbital floor fractures with stable ledges are most suitable for endoscopic techniques. Because it involves minimal globe manipulation, the endoscopic approach may be appropriate in patients in whom traditional approaches are contraindicated, such as those with hyphema, retinal detachment, or globe injuries.
Limitations and Contraindications
Relative contraindications to repair of orbital fractures are mostly related to ocular injuries (e.g., hyphema, globe ruptures, retinal tears) and recent ophthalmologic surgery. Ophthalmologic evaluation and clearance are warranted in these cases before surgery is considered. Additional relative contraindications include patients who have vision only in the affected orbit/eye and life-threatening instability.
The same contraindications to the traditional approach apply to the endoscopic approach. However, an advantage of the latter is that endoscopic-assisted orbital repair surgery can be done earlier in some ocular injuries because the minimally invasive nature of the procedure requires less eye manipulation. Endoscopic repair of a large two-wall orbital defect is contraindicated because the implant is more difficult to stabilize.
As with any endoscopic approach, it is important to discuss with the patient the possibility that a traditional approach may have to be used if the endoscopic repair is unsuccessful.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


