Introduction
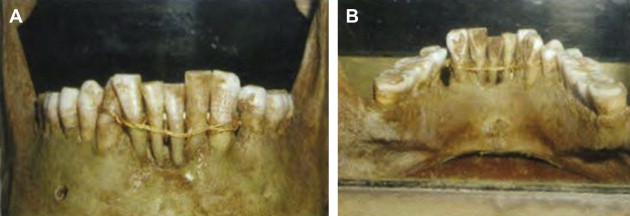
Literature specific to dental alveolar trauma and treatment dates back as far as the Greco-Roman period (350 bc to ad 750). Hippocrates was the first to document dental alveolar treatment regimens in his writings. The concept of bridle wiring and reestablishing proper occlusion was alluded to during these early times ( Fig. 1 ).
The causes of dental alveolar trauma are specific for age, sex, and demographics.
-
Age:
- •
Pediatric group: trauma is usually a result of falls associated with the gross weight disparity between anatomic development and skeletal weight distribution (big heads with small bodies). This type of trauma is usually seen in children aged between 2 and 4 years.
- •
Children in the primary dentition stage have an overall prevalence of dental alveolar trauma reaching 30%.
- •
Children in the mixed dentition stage have a prevalence of trauma ranging from 5% to 20%.
- •
Contact sports and child’s play results in most of the dental alveolar trauma seen in children and adolescents.
- •
Child abuse is quoted in the literature as another cause of dental alveolar trauma. In the United States, more than 50% of child abuse involves trauma to the head and neck region, and internationally, 7% of injuries involve the oral cavity.
- •
Dental alveolar trauma in adults may involve contact sports, assaults, and motor vehicle accidents.
-
Sex:
- •
Men are twice as likely to sustain dental alveolar trauma (2:1).
-
Demographic:
- •
Most orofacial injuries resulted from intentional violence and involved primarily socially and economically disadvantaged groups in minority populations.
- •
Medically or psychologically challenged patients tend to be at higher risk (ie, mental, seizure, and congenital maxillofacial abnormalities).
- •
The most frequent general anesthesia-related litigation claim involved damage to teeth.
- •
Inadequate laryngoscopy technique and the increased biting forces seen in comatose patients are another cause of dental alveolar injury ( Fig. 2 ).



