1 Occlusion and malocclusion
Ideal occlusion
The ideal relationship of the teeth can be defined in terms of static (or morphological) and functional occlusion. Edward Angle (Box 1.1) felt the key to normal occlusion was the relative anteroposterior position of the first permanent molars, which he used to define the dental arch relationship. He also recognized the importance of good cuspal interdigitation to provide mutual support for the teeth in function (Angle, 1899). Almost one hundred years after Angle, Lawrence Andrews redefined the concept of an ideal static occlusion by describing it in terms of six individual keys, including an updated ideal relationship for the first molars (Andrews, 1972) (Box 1.2).
Orthodontists have traditionally based their treatment upon these static goals, with little consideration for the dynamics of occlusion or temporomandibular joints and associated musculature that forms the masticatory system. However, over the past few decades there has been a greater interest in the principles of gnathology and aspects of an occlusion in function (Table 1.1). Much has been written about what constitutes an ideal functional occlusion and why it is important (Box 1.3); however, an essential concept is one of mutual protection, whereby teeth of the anterior and posterior dentitions protect each other in function. Mutual protection is thought to be achieved in the presence of:
Box 1.3 How important is an ideal functional occlusion?
Advocates of an ideal functional occlusion claim it is necessary to avoid temporomandibular dysfunction, periodontal breakdown and long-term occlusal instability. Indeed, it has been suggested that orthodontic treatment is indicated in all young adults in whom the occlusion is not functionally optimal. These criteria would mean treating most of the population, as an ideal functional occlusion is not very common. For example, as many as 75% of subjects have been described as having non-working side contacts (Tipton & Rinchuse, 1991), whilst a difference of greater than 2 mm has been reported between RCP and ICP for up to 40% of orthodontic patients (Hidaka et al., 2002). So does this matter? Whilst artificially creating non-working side interferences can increase the signs and symptoms of temporomandibular dysfunction (Christensen and Rassouli, 1995), the results of occlusal equilibration, when an idealized functional occlusion is created, are equivocal. Canine guidance has been reported to reduce electromyographic (EMG) activity of the muscles of mastication (Christensen and Rassouli, 1995) but the reproducibility of EMG is open to question (Cecere et al., 1996). There does appear to be a relationship between temporomandibular dysfunction and large slides from RCP into ICP (Solberg et al., 1979) although the correlations between other traits of malocclusion and temporomandibular dysfunction are generally weak (Egermark-Eriksson et al., 1981). So by treating to an ideal functional occlusion does it eliminate or reduce temporomandibular dysfunction? Unfortunately, there is a lack of evidence to support this, or the claim that it results in greater long-term stability ( Luther, 2007a, b). Therefore, while any treatment should aim for an ideal functional occlusion, if it is not achieved, there do not appear to be long-term serious consequences to the patient.
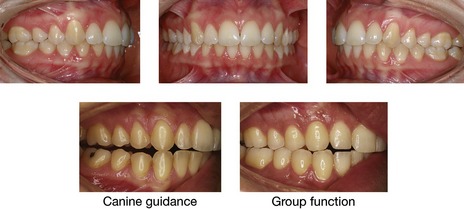
In reality, an ideal static or functional occlusion is rarely found in Western societies (Fig. 1.1), which have a high occurrence of various traits of malocclusion.
Classification of malocclusion
Molar classification
Angle classified occlusion according to the molar relationship and this remains the most internationally recognized classification of malocclusion. When looking at ideal occlusion, Angle found that the mesiobuccal cusp of the upper first permanent molar should occlude with the sulcus between the mesial and distal buccal cusps of the lower first permanent molar (Fig. 1.2). He therefore based his classification of occlusion on this relative mesiodistal position:
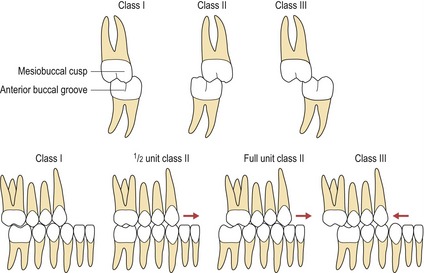
In clinical practice, it is common to describe molar relationships in terms of half or even a third of a tooth unit of a class II or class III relationship (Fig. 1.2). However, a basic premise of the Angle classification is that the first permanent molars hold a fixed position within the dental arch, which is not necessarily the case. Early loss of deciduous teeth can influence their position and distort the molar relationship and this classification can also be difficult to apply when there is an asymmetric molar relationship. These problems can lead to low levels of inter-examiner agreement (Gravely and Johnson, 1974).
Canine classification
The canine relationship also provides a useful anteroposterior occlusal classification:
Similarly to the molar relationship, the severity of the canine relationship can also be described in terms of tooth units and can be inappropriately influenced by local factors such as crowding (Fig. 1.2).
Incisor classification
A more clinically relevant method of classifying malocclusion is based upon the relationship of the maxillary and mandibular incisors. This represents a truer reflection of the underlying skeletal base relationship and also highlights what is often of most concern to the patient. It is essentially the Angle classification, as applied to the incisor teeth, and is defined upon the relationship of the mandibular incisor tip to the cingulum plateau of the maxillary central incisors (Fig. 1.3), being included in the British Standards Institute’s Glossary of Dental Terms:
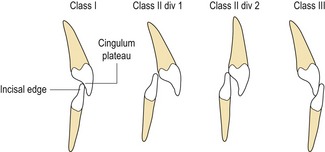
Confusion can arise when the upper incisors are upright or retroclined, but with an increased overjet. This has led to the introduction of a class II intermediate classification (Williams and Stephens, 1992):
Prevalence of malocclusion
Malocclusion has been described as a disease of Western societies, and certainly within developed polygenic societies, certain occlusal traits such as crowding are more common. Indeed, from data generated by population studies, the presence of one or more traits of malocclusion is very common. In the USA, noticeable incisor irregularity is present in the majority of adults, with only 34% having well-aligned mandibular incisors and 45% well-aligned maxillary incisors. In addition, about 20% of the American population has a marked deviation from the ideal sagittal jaw relationship, with 2% of these being disfiguring and at the limit for orthodontic correction (Proffit et al, 1998). Within the UK, the last Child Dental Health Survey found around 35% of 12 year olds with a definite need for orthodontic treatment on dental health or aesthetic grounds, which increased to 43% when those already in treatment were included (Chestnutt et al, 2006).
Aetiology of malocclusion
A malocclusion should be regarded as a developmental condition and does not represent a single entity. Rather, it is the sum of a number of complex occlusal traits, which demonstrate multifactorial inheritance. Although in certain cases specific factors and pathologies can be identified as the cause of a malocclusion; in the majority, the aetiology is less clear. In each individual there is a close interaction between genetics and the environment during development and growth of both the jaws and dentition; it is at this interface that the aetiology of malocclusion lies (Box 1.4).
Evolutionary trends
Comparison of large population studies with archaeological records confirms that malocclusion has become more common over the past 1000 years. In fact, epidemiological data show that the increase in human occlusal variation has been rapid, taking place within a couple of generations, occasionally even from one generation to the next (Weiland et al, 1997). A rapid change such as this would imply a significant contribution from a changing environment, such as has occurred with increasingly urbanized and industrialized societies (Corruccini, 1984). It has been hypothesized that dietary changes in modern societies, with increased consumption of soft, energy-rich food, has resulted in less interproximal wear between the teeth. Research on aboriginal and stone aged populations has demonstrated this lack of attrition as a possible cause of malocclusion, particularly crowding (Begg, 1954). However, it has been shown that the amount of tooth material lost in each quadrant by interproximal wear is not more than 2 to 3-mm (Fig. 1.4).

A soft diet may also result in underdevelopment of the jaws and a lack of arch space, leading to crowding. According to this hypothesis, hard diet requires vigorous mastication, stimulating the growth of facial bones, particularly in the transverse dimension of the maxilla and mandible. Tooth wear is merely a by-product, brought about by diet-related attrition and high masticatory activity, and has only a minor effect on tooth alignment. Experimental studies have shown that dietary consistency and masticatory activity affect not only the masticatory muscles, but also many aspects of bone growth, including bone size and mass, internal bone structure, and craniofacial size and morphology (Varrela, 2006).
Genetic influences
Until recently, most information on the relative contribution of genetic factors to malocclusion has been gained from family studies and the twin method. Monozygotic twins are genetically identical, whereas dizygotic twins only share 50% of their genetic makeup. Therefore, by comparing the differences in occlusal traits between pairs in both groups, some indication of the genetic influence on a particular trait is given; the larger the difference, the greater the genetic effect (Corruccini et al, 1990). This assumes that the environmental effects are similar for both groups.
Many developmental dental anomalies have been shown to occur together and have a strong familial trend. An example of this is development of a palatally impacted maxillary canine, which is more common in females and certain ethnic groups and is often associated with microdont or absent lateral incisors (Peck et al, 1994). Similarly, jaw growth appears to be mostly genetically determined. A higher correlation has been shown between patients and immediate family than in unrelated subjects for class II division 1 malocclusion, which supports a polygenetic inheritance, particularly in relation to mandibular retrognathia. However, environmental factors, such as lower lip position and digit sucking, can also play a part. Mandibular prognathism, found in class III malocclusions, seems to have a high genetic predisposition, as demonstrated by the high familial inheritance and variation amongst different ethnic groups. More robust evidence for this exists from studies of siblings and first degree relatives (Litton et al, 1970; Watanabe et al, 2005).
Dental arch size and form seems to be more subject to environmental influences (Cassidy et al, 1998). Dental crowding represents a discrepancy between the size of the teeth and the size of the dental arch. Tooth development, including the size, form and presence of teeth within a dentition, is under strong genetic influence. However, the main aetiological factor in crowding appears to be arch size as opposed to tooth size (Howe et al, 1983).
Large population studies have also investigated the influence of population admixture and inbreeding on malocclusion. Generally, the results of these epidemiological studies have shown a greater genetic influence on skeletal relations and arch size and a lower heritability of dental variables such as overbite, molar relationships and crowding, suggesting a greater environmental influence. The importance of hereditary factors also appears to increase with severity of the malocclusion. Although craniofacial form and growth may be under genetic control, the reason that siblings often present with similar malocclusions is probably related to their similar responses to environmental influences. Therefore, while malocclusion appears to be acquired, the underlying genetic control of craniofacial form will tend to divert siblings into similar physiological responses, resulting in the development of similar malocclusions (King et al, 1993).
These studies have also shown that malocclusion does not follow simple Mendelian inheritance, but rather polygenetic or epigenetic transmission, when the interaction of genes with each other and the environment during development determine the phenotypic variation of the trait. Therefore, each would have an additive effect, showing variation along a continuous scale for traits of a malocclusion, which is exactly what happens. Theoretically, in genetically isolated communities, alleles for these traits may be expressed more frequently, giving an indication which have a greater genetic component. Island studies investigating the effects of inbreeding on malocclusion support this polygenetic theory of transmission for certain traits such as overjet and overbite (Lauc et al, 2003).
Environmental factors
The developing dentition is under the influence of resting soft tissue pressure form, and function: lying in a position of muscular balance or equilibrium (Proffit, 1978). Teeth erupt under the influence of the lips and cheeks on one side and the tongue on the other. Abnormal soft tissue patterns seen in those with persistent digit-sucking habits or lip incompetence, with the lower lip trapped behind the upper incisors in function, may predispose to an increased overjet. An alteration in tooth position can also arise when there is a change in this balance of force. Possible causes may be physiological, habitual or pathological and may impact on the lips, cheeks, tongue and periodontal tissues.
Physiological factors
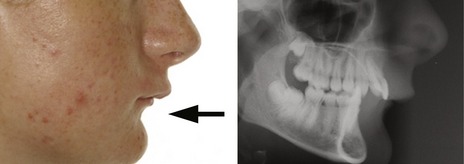
A physiological adaptation can take place in the presence of a skeletal base discrepancy. When teeth erupt, they do so under the influence of soft tissue pressure from the lips, cheeks and tongue. There is a tendency, most notably in the labial segments, for them to upright or procline towards teeth in the opposing arch. This is most often seen in class III skeletal cases, with proclination of the upper incisors and retroclination of the lowers (Fig. 1.5).

Soft tissue envelope


Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


