This article reports the successful use of miniscrews in the mandible to treat a 20-year-old Mongolian woman with a chief complaint of anterior crossbite. The patient had a skeletal Class III malocclusion with a mildly protrusive mandible, an anterior crossbite, and a deviated midline. In light of the advantages for reconstruction of the occlusal plane and distal en-masse movement of the mandibular arch, we used a multiloop edgewise archwire in the initial stage. However, the maxillary incisors were in excessive labioversion accompanied by little retraction of the mandibular incisors; these results were obviously not satisfying after 4 months of multiloop edgewise archwire treatment. Two miniscrews were subsequently implanted vertically in the external oblique ridge areas of the bilateral mandibular ramus as skeletal anchorage for en-masse distalization of the mandibular dentition. During treatment, the mandibular anterior teeth were retracted about 4.0 mm without negative lingual inclinations. The movement of the mandibular first molar was almost bodily translation. The maxillary incisors maintained good inclinations by rotating their brackets 180° along with the outstanding performance of the beta-titanium wire. The patient received a harmonious facial balance, an attractive smile, and ideal occlusal relationships. The outcome was stable after 1 year of retention. Our results suggest that the application of miniscrews in the posterior area of the mandible is an effective approach for Class III camouflage treatment. This technique requires minimal compliance and is particularly useful for correcting Class III patients with mild mandibular protrusion and minor crowding.
Smile attractiveness has been regarded as a standard of successful treatment by both orthodontists and patients. Evaluating the face in the smiling profile is also a critical part of a complete orthodontic diagnosis. Maxillary incisors play an important role in defining beauty, and thus they should be angulated and positioned most favorably in their anteroposterior and vertical relationships to all facial structures to ensure maximum facial harmony. Excessive labioversion of the maxillary incisors can easily ruin a pleasing smile.
Dentoalveolar compensations (proclined maxillary incisors and retroclined mandibular incisors) are common in patients with a Class III malocclusion caused by a retrognathic maxilla or a prognathic mandible. Also, moderate proclination of the maxillary incisors is indispensable in camouflage treatment of anterior crossbite. It is always, therefore, challenging for orthodontists to place the maxillary incisors in an appropriate anteroposterior position with a harmonious labial inclination in Class III treatment. To prevent excessive proclination of the maxillary incisors, distal en-masse movement of the mandibular dentition is quite effective in camouflage treatment for patients with a Class III malocclusion. The multiloop edgewise archwire is considered a practical method with fewer side effects. However, the extent of occlusal enhancement that occurs in response to the multiloop edgewise archwire greatly depends on a patient’s compliance and can vary with each person. As skeletal anchorage, the application of miniscrews, which offer more simple and stable force systems, has gradually become popular and reliable.
In this case report, we introduce a nonsurgical treatment of an adult with a Class III malocclusion with miniscrew-assisted mandibular dentition distalization. At the beginning of the therapy, the multiloop edgewise archwire technique resulted in an unsatisfying smile because of the excessive proclination of the maxillary incisors. Then we stopped to vertically implant a pair of miniscrews in the external oblique ridge areas of the bilateral mandibular ramus as anchorage for the distal en-masse movement of the mandibular dentition and obtained an excellent treatment outcome ultimately.
Diagnosis and etiology
The patient was a 20-year-old Mongolian woman who had a Class III facial type and slight crowding with a complete Class III relationship. Her chief complaint was an anterior crossbite. Her medical history showed no contraindication for orthodontic therapy, and no one in her direct family had skeletal Class III features.
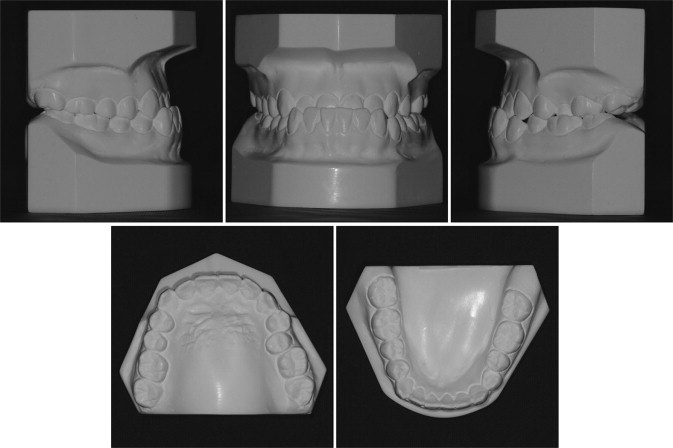
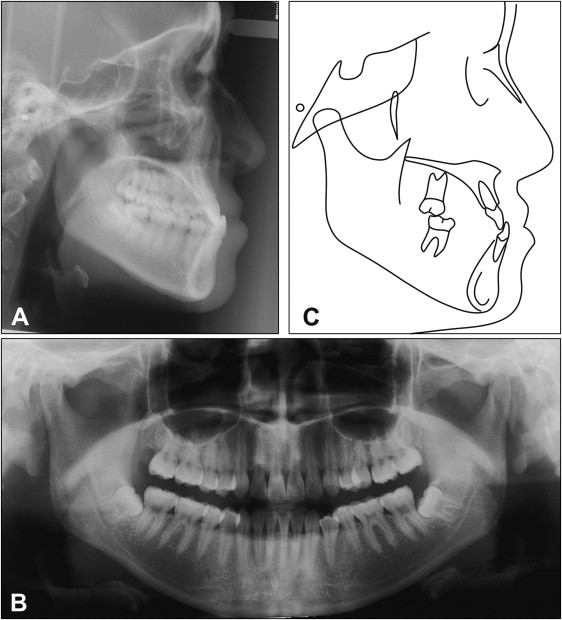
The photographs taken before treatment showed symmetric facial structures ( Fig 1 ). The patient had a concave facial profile, a protrusive lower lip, and an acute nasolabial angle. Her maxillary anterior teeth were retrognathic, with inadequate display when smiling. The mandibular dental midline was deviated 2.0 mm to the right, although the maxillary dental midline was coincident with the facial midline. There were no signs or symptoms of temporomandibular joint dysfunction. Mandibular movements, such as maximal opening and lateral and anterior displacement, were within normal limits. No deviation and pain were discovered during the border movement of the mandible. The dental casts ( Fig 2 ) showed a Class III occlusion on each side, without apparent crowding. Overjet was −2.0 mm, and overbite was −4.5 mm. A cephalogram ( Fig 3 , A ) and a panoramic radiograph ( Fig 3 , B ) were taken before treatment. The cephalometric analysis ( Table ) and its tracing ( Fig 3 , C ) showed that the mandible protruded relative to the cranial base (SNB angle, 81.7°; ANB angle, −2.6°). The panoramic radiograph ( Fig 3 , B ) showed no other abnormal signs, except that the 2 germs of the mandibular third molars were tipped mesially.

| Measurement | Pretreatment | After 4 months of multiloop edgewise archwire treatment | Posttreatment |
|---|---|---|---|
| SNA (°) | 79.1 | 77.8 | 77.6 |
| SNB (°) | 81.7 | 79.2 | 79.1 |
| ANB (°) | −2.6 | −1.4 | −1.5 |
| SN-GoGn (°) | 36.1 | 39.0 | 38.9 |
| S-Go/N-Me (%) | 61.3 | 59.4 | 59.4 |
| FH-OP (°) | 9.9 | 8.7 | 6.6 |
| U1-SN (°) | 79.6 | 64.7 | 77.7 |
| L1-NB (°) | 18.4 | 24.0 | 13.5 |
After the analysis of the photographs, casts, and radiographs, it was decided to approach her problems as a skeletal Class III malocclusion with an anterior crossbite and a deviated midline.
Treatment objectives
The treatment objectives were to (1) obtain a harmonious facial profile by decreasing the protrusion of the mandible; (2) improve the occlusion, including correction of the anterior crossbite, establishment of ideal overjet and overbite, and achievement of Class I molar relationships; and (3) place the dental midlines in the middle of the patient’s face.
Treatment objectives
The treatment objectives were to (1) obtain a harmonious facial profile by decreasing the protrusion of the mandible; (2) improve the occlusion, including correction of the anterior crossbite, establishment of ideal overjet and overbite, and achievement of Class I molar relationships; and (3) place the dental midlines in the middle of the patient’s face.
Treatment alternatives
The first alternative was combined surgical and orthodontic treatment. The anterior crossbite would be corrected with a mandibular setback, and the concave profile would be improved as well. However, we decided that her skeletal problem was not sufficiently excessive to require orthognathic surgery.
The second alternative was orthodontic treatment with extraction of 4 premolars. Through the retraction of the mandibular anterior teeth and the mesial movement of the maxillary molars, the anterior crossbite and Class III molar relationships would be corrected, and the concave facial profile would be camouflaged. Nevertheless, her mandibular incisors were not suitable for much distal movement because of the thin trabecular bone in the mandibular anterior area that could damage the periodontal tissues by gingival recession, fenestration, or dehiscence.
The third alternative was to extract the mandibular third molars and use the multiloop edgewise archwire technique to obtain distal en-masse movement of the mandibular arch with short Class III elastics. Thereby, the anterior crossbite would be corrected, the molar relationships would be changed into Class I, and her concave facial profile would be camouflaged as well.
After we discussed the 3 alternatives with the patient, she chose the third option and promised to cooperate in extracting the third molars and wearing the Class III elastics.
Treatment progress
Orthodontic treatment began on November 9, 2007. The mandibular third molars were extracted before bonding. Preadjusted 0.022-in brackets (Shiye, Hangzhou, China) were bonded to all teeth. Alignment and leveling with sequential nickel-titanium archwires were achieved in 12 months, ending with 0.018 × 0.025-in stainless steel wires. After that, 0.018 × 0.025-in stainless steel multiloop edgewise archwires with progressive tip-back bends were placed in both arches. The patient was instructed to wear the short Class III elastics (3/16 in, 6 oz; 3M Unitek, Monrovia, Calif) for 24 hours per day ( Fig 4 , A ).


