Introduction
The objective of this study was to evaluate natural changes in maxillary posterior alveolar height (MPAH) and axial inclination of the maxillary first molars (AIMFM) in subjects with Class II malocclusion to determine the validity of predictive equations.
Methods
Longitudinal records of 30 untreated white subjects (13 girls, 17 boys) with skeletal Class II malocclusion were collected at ages 9, 12, 14, and 16 years. They had participated in the Burlington Growth Centre study, and cephalograms were analyzed with Dentofacial Planner Plus software (version 2.0, Dentofacial Planner, Toronto, Ontario, Canada). Serial means were compared with the Bonferroni post-hoc test ( P <0.05). Predictive equations were obtained and studied with the analysis of agreement.
Results
Gradually, means of MPAH had statistical increments with sexual dimorphism from 14 to 16 years of age. A distal mean of AIMFM was found at 9 years of age that decreased significantly during growth, with sexual dimorphism between the ages of 9 and 12 years. Changes in AIMFM varied among subjects in distinct stages. Values of MPAH were predicted with high validity at intervals of 3 years or longer, whereas estimations for AIMFM were unreliable.
Conclusions
In this study group, there was significant alveolar growth, with a natural tendency to upright the distal inclination at the maxillary first molars.
Class II malocclusions have been successfully corrected with headgear appliances, mandibular advancers, and premolar extractions. Each approach is indicated for specific conditions of this malocclusion. In severe cases, treatment results are improved with orthognathic surgery. During puberty, headgears have shown results with orthopedic effects, controlled by the vector of forces. However, undesirable extrusion or distal tipping of the maxillary first molars has also been noted after treatment with cervical headgear and other appliances. Natural growth changes of the maxillary first molars indicate that these aspects are not completely caused by mechanics.
After the resorption of the deciduous dental roots, significant remodeling of the alveolar process occurs, and new alveolar bone is formed to support the newly erupted teeth. Increments of maxillary posterior alveolar height are reported in early and late stages of pubertal growth, with its magnitude varying proportionally in different facial types. Moreover, changes in the axial inclination of maxillary first molars can occur with alveolar growth, even if no mesial inclination of these molars is noted in patients with maxillary protrusion on both alveolar and basal bones. In this scenario, the vertical height of the maxillary molars has been analyzed to predict changes in the mandibular plane ; the intermolar angle is also used with other references to predict mandibular rotation.
The importance of the maxillary molars’ height and axial inclination in the variations of the mandibular plane has been recognized. However, the contribution of physiologic and mechanical factors to the severity of undesirable results needs to be investigated. Rarely are growth changes considered in the analysis of molar tipping or extrusion after treatment. In 1957, Klein suggested an urgent need for serial investigation of untreated Class II subjects to evaluate growth increments per year, because of differences in the times of treatment. Therefore, the following questions should be answered. How much vertical growth can be expected in maxillary posterior alveolar height? What is the natural pattern of changes in the axial inclination of the maxillary first molars? Is the stage of growth important in the variability of changes? The objectives of this study were to answer these questions and determine predictive equations for natural changes and their validity.
Material and methods
Thirty untreated white subjects (13 girls, 17 boys) with Class II malocclusion, who had normal development of the dentition with no missing permanent teeth and no evident metabolic diseases, were selected from the files of the Burlington Growth Centre. Serial records comprised lateral cephalograms and clinical remarks at ages 9, 12, 14, and 16 years. Skeletal maturation was assessed on hand-wrist radiographs according to the standards of Greulich and Pyle. Differences between chronologic and skeletal ages did not exceed 2 years in either direction. After the cephalograms were manually traced, landmarks were digitized and studied with Dentofacial Planner Plus software (version 2.0, Dentofacial Software, Toronto, Ontario, Canada).
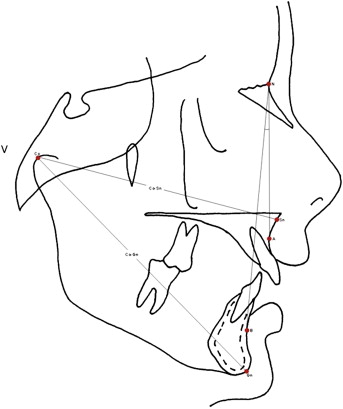
Subjects were included in this study if skeletal Class II malocclusion was characterized at age 12 years, as follows: ANB angle equal to or above 5° or a linear difference between the mandibular length (condylion to gnathion, CoGn) and the middle third of the face (condylion to subnasale, CoSn) equal to or less than 20 mm ( Fig 1 ). The palatal plane (PP) was located, and a perpendicular line was traced ( Fig 2 ) from there to the tip of the mesiobuccal cusp of the maxillary left first molar (tcMFM). The distance between PP and tcMFM (PP-tcMFM), and the axial inclination of this molar (axMFM) in relation to the PP (PP-axMFM) were both measured ( Fig 2 ). The analysis of intraexaminer error was made as previously described, corroborating the reliability of the measurements.
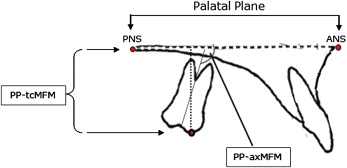
By measuring PP-tcMFM (millimeters) and PP-axMFM (degrees) at ages 9, 12, 14, and 16 years, means of maxillary posterior alveolar height (MPAH) and axial inclination of the maxillary first molar (AIMFM) were obtained, respectively. Growth changes were calculated by the difference between values measured in later and earlier ages. Serial measurements of MPAH and AIMFM were correlated, and the derived regressive equations were used to predict growth changes in distinct stages. A second equation was obtained to simplify the predictions, when the intercept point was arbitrarily defined as zero (a = 0).
Statistical analysis
Means of serial ages and consecutive changes of growth were analyzed separately, by using analysis of variance (ANOVA) with the Bonferroni post-hoc test ( P <0.05). Sexual dimorphism was evaluated with the Student t test ( P <0.01). Predicted means for corresponding ages were compared with each other and with the actual mean by using 1-way ANOVA ( P <0.05). Squared multiple correlation (R 2 ), mean of error, and coefficient of accuracy were calculated for predictions.
The subjects’ increasing MPAH and the frequency of each pattern of changes on AIMFM were assessed in consecutive stages of growth. Changes of MPAH were classified as incremental, if the difference between the ending and starting values was greater than 0.2 mm; or nonincremental, if this difference was equal to 0 ± 0.2 mm. The pattern of changes in AIMFM was defined as mesial tipping, if angle PP-axMFM decreased from the starting to ending age (≤0.5°); or distal tipping, if this value increased along the stage of growth (>0.5°). A subject’s overall change in AIMFM was considered in each stage when the difference was 0° ± 0.5°. Predicted changes were also classified into the same criteria and the agreement between agreement between predicted and actual changes was analyzed in both variables, MPAH and AIMFM. In this analysis, the validity of the predictions was determined by the level of confidence, considered high if agreement was equal or greater than 90%.
Results
Means of MPAH and AIMFM at ages 9, 12, 14, and 16 years were calculated; there was no sexual dimorphism ( Table I ). Significant increases in MPAH were noted in intervals of 3 years or longer ( Table I ). Overall growth was statistically greater than in shorter stages ( Table II ), and incremental changes were greater in boys from 14 to 16 years of age ( Table II ). Four years of growth were necessary to identify statistical difference between means of AIMFM in serial ages ( Table I ). The maxillary first molars had distal crown inclinations at age 9 years with a tendency to upright gradually until age 16 ( Table I ). Overall changes in AIMFM were greater than in shorter stages, and sexual dimorphism was noted from 9 to 12 years of age ( Table II ). Natural changes in AIMFM from 9 to 12 years were statistically greater than in the stage between 12 and 14 years ( Table II ).
| 9 years | 12 years | 14 years | 16 years | |
|---|---|---|---|---|
| MPAH (mm) | ||||
| PP-tcMFM | 17.8 ± 1.9 a | 20.0 ± 2.2 b | 21.4 ± 2.5 c | 22.7 ± 2.6 d |
| Girls | 17.7 ± 1.4 | 20.1 ± 1.9 | 21.7 ± 2.5 | 22.3 ± 2.2 |
| Boys | 17.9 ± 2.2 | 19.8 ± 2.5 | 21.3 ± 2.6 | 23.0 ± 2.9 |
| AIMFM (°) | ||||
| PP-axMFM | 102.4 ± 5.3 e | 99.1 ± 5.6 f | 96.3 ± 6.0 g | 94.4 ± 6.1 h |
| Girls | 103.8 ± 5.2 | 97.8 ± 6.9 | 96.5 ± 8.1 | 94.7 ± 7.7 |
| Boys | 101.4 ± 5.3 | 100.0 ± 4.5 | 96.1 ± 4.0 | 94.1 ± 4.9 |
| 9-12 y | 12-14 y | 14-16 y | 9-16 y | |
|---|---|---|---|---|
| MPAH (mm) | ||||
| PP-tcMFM | 2.2 ± 1.3 a | 1.5 ± 1.3 a | 1.2 ± 1.3 a | 4.9 ± 1.6 b |
| Girls | 2.5 ± 1.1 | 1.5 ± 1.2 | 0.6 ± 0.9 ∗ | 4.6 ± 1.2 |
| Boys | 1.9 ± 1.4 | 1.4 ± 1.4 | 1.7 ± 1.4 ∗ | 5.1 ± 1.9 |
| AIMFM (°) | ||||
| PP-axMFM | –3.4 ± 5.7 c | –2.8 ± 4.3 d | –1.9 ± 3.8 e | –8.1 ± 6.1 f |
| Girls | –6.0 ± 4.5 ∗ | –1.3 ± 5.1 | –1.8 ± 5.0 | –9.1 ± 5.7 |
| Boys | –1.4 ± 5.9 ∗ | –3.9 ± 3.2 | –1.9 ± 2.7 | –7.3 ± 6.4 |
Correlations were strong for MPAH ( Table III ), and the equations showed high values of R 2 (0.58-0.76), low means of error, and low coefficients of accuracy ( Table III ). The overall correlation of AIMFM was fairly weak, contrasting with higher values in later stages ( Table IV ). Predictions for AIMFM showed high means of error and weak R 2 values; these were higher from 14 to 16 years of age ( Table IV ). Nevertheless, there were no statistical differences when we compared the predicted means with the actual values of MPAH and AIMFM ( P >0.05).
| Stage of growth (y) | Correlation | Regressive equation | R 2 | Predicted mean (mm) | Mean of error (mm) | Coefficient of accuracy (mm) |
|---|---|---|---|---|---|---|
| 9-12 | .82 | Y = 0.98X + 2.5 | .67 | 20.0 + 1.8 | 0.0 + 1.3 | .065 |
| Y 0 = 1.12X | .65 | 20.0 + 2.1 | 0.0 + 1.3 | .065 | ||
| 9-14 | .77 | Y = 1.05X + 2.75 | .59 | 21.5 + 2.0 | 0.0 + 1.6 | .075 |
| Y 0 = 1.2X | .58 | 21.4 + 2.2 | 0.1 + 1.6 | .079 | ||
| 12-14 | .87 | Y = 0.99X + 1.7 | .75 | 21.5 + 2.2 | 0.0 + 1.3 | .061 |
| Y 0 = 1.07X | .74 | 21.4 + 2.4 | 0.1 + 1.3 | .065 | ||
| 9-16 | .79 | Y = 1.11X + 2.8 | .63 | 22.6 + 2.1 | 0.1 + 1.6 | .075 |
| Y 0 = 1.27X | .61 | 22.6 + 2.4 | 0.1 + 1.6 | .075 | ||
| 12-16 | .86 | Y = 1.003X + 2.6 | .73 | 22.6 + 2.2 | 0.1 + 1.3 | .062 |
| Y 0 = 1.13X | .72 | 22.6 + 2.5 | 0.1 + 1.4 | .066 | ||
| 14-16 | .87 | Y = 0.89X + 3.4 | .76 | 22.5 + 2.3 | 0.2 + 1.3 | .067 |
| Y 0 = 1.056X | .74 | 22.6 + 2.7 | 0.0 + 1.3 | .058 |
| Stage of growth (y) | Correlation | Regressive equation | R 2 | Predicted mean (°) | Mean of error (°) | Coefficient of accuracy (°) |
|---|---|---|---|---|---|---|
| 9-12 | .45 | Y = 0.48X + 49.8 | .20 | 99.0 + 2.6 | –0.1 + 5.0 | –.052 |
| Y 0 = 0.96X | –.004 | 98.3 + 5.1 | –0.7 + 5.6 | –.064 | ||
| 9-14 | .44 | Y = 0.49X + 45.5 | .19 | 95.7 + 2.6 | –0.6 + 5.4 | –.063 |
| Y 0 = 0.94X | .04 | 96.3 + 5.0 | 0.0 + 5.9 | .061 | ||
| 12-14 | .73 | Y = 0.77X + 19.7 | .53 | 96.0 + 4.3 | –0.3 + 4.1 | –.046 |
| Y 0 = 0.97X | .49 | 96.1 + 5.5 | 0.2 + 4.2 | –.046 | ||
| 9-16 | .44 | Y = 0.5X + 42.4 | .19 | 93.6 + 2.7 | –0.8 + 5.5 | –.067 |
| Y 0 = 0.92X | .06 | 94.2 + 4.9 | –0.1 + 5.9 | –.064 | ||
| 12-16 | .76 | Y = 0.83X + 12.0 | .58 | 94.2 + 4.7 | –0.2 + 4.0 | –.045 |
| Y 0 = 0.95X | .57 | 94.1 + 5.4 | –0.3 + 4.0 | –.046 | ||
| 14-16 | .80 | Y = 0.83X + 14.9 | .65 | 94.8 + 5.0 | 0.4 + 3.6 | .042 |
| Y 0 = 0.98X | .62 | 94.3 + 5.8 | 0.0 + 3.8 | .040 |
Although incremental changes were found in all 30 subjects, half had 1 stage without natural increases ( Table V ): 3 boys between ages 9 and 12 years, 4 boys and 2 girls from 12 to 14 years, and 4 girls and 2 boys between 14 and 16 years. The frequency of increasing MPAH was high in 3-year intervals or longer periods of growth ( Table V ). Agreement between the predicted and actual changes on MPAH was high from 9 years to 12, 14, and 16 years of age. It was also high between ages 12 and 16 years ( Table V ). When a nonincremental stage was experienced, increases in MPAH were predicted with equations ( Table V ). Overall changes on AIMFM showed a high frequency of mesial tipping contrasting with a low percentage found in shorter stages ( Table VI ). One period without natural changes in AIMFM was identified in 3 subjects, whose overall pattern was mesial tipping. Agreement between predicted and actual changes in AIMFM was high only for the overall period ( Table VI ).
| Stage of growth prediction (y) | Growth changes | Agreement (prediction /actual) | |
|---|---|---|---|
| Incremental | Nonincremental | ||
| 9-12 | |||
| Agreed | 27 | – | 27 (90%) |
| Disagreed | – | 3 | 3 (10%) |
| Actual frequency | 27 (90%) | 3 (10%) | 30 (100%) |
| 9-14 | |||
| Agreed | 30 | – | 30 (100%) |
| Disagreed | – | – | 0% |
| Actual frequency | 30 (100%) | 0% | 30 (100%) |
| 12-14 | |||
| Agreed | 24 | – | 24 (80%) |
| Disagreed | – | 6 | 6 (20%) |
| Actual frequency | 24 (80%) | 6 (20%) | 30 (100%) |
| 9-16 | |||
| Agreed | 30 | – | 30 (100%) |
| Disagreed | – | – | 0% |
| Actual frequency | 30 (100%) | 0% | 100% |
| 12-16 | |||
| Agreed | 30 | – | 30 (100%) |
| Disagreed | – | – | 0% |
| Actual frequency | 30 (100%) | 0% | 30 (100%) |
| 14-16 | |||
| Agreed | 24 | – | 24 (80%) |
| Disagreed | – | 6 | 6 (20%) |
| Actual frequency | 24 (80%) | 6 (20%) | 30 (100%) |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


