An adolescent girl with an Angle Class III malocclusion, excessive lower facial height, and anterior open bite sought nonsurgical treatment. She was treated with a multiloop edgewise archwire (MEAW). In association with a chincup, MEAW mechanics allowed the successful correction of the anterior open bite and the molar relationship, without major alterations of the patient’s profile. Combined orthodontic and surgical treatment should be considered for patients with skeletal anterior open-bite malocclusion. For patients who do not want surgery, however, MEAW treatment is an alternative that can have excellent results.
An anterior open bite malocclusion is a difficult problem in orthodontic treatment. Because of separate occlusal planes for the maxillary and mandibular dentitions, the open bite would be configured by the anterior divergence of these planes, instead of the overlap seen in normal occlusion. This malocclusion is usually associated with internal derangement of the temporomandibular joint.
Most patients with anterior open bites have both a dentoalveolar component and increased skeletal vertical dimension. The true skeletal open-bite patient would require a combination of orthodontic treatment and orthognathic surgery to achieve a stable occlusion, acceptable esthetics, and improved function. However, surgery can be too expensive for some patients, and others refuse to consider such an invasive intervention. The orthodontist’s only choice will be to deny treatment or try to resolve as much of the malocclusion as possible with orthodontic treatment alone.
The multiloop edgewise archwire (MEAW) was introduced by Kim ; he had already been using it for almost 2 decades. This technique has been successfully applied for treatment of severe open-bite malocclusions. The objectives of treatment include proper vertical positioning of the maxillary incisors, compatible cant of the maxillary and mandibular occlusal planes, and uprighted inclination of the posterior teeth. The form of the MEAW is primarily that of an ideal edgewise archwire with the addition of boot loops. The vertical loop component serves as a break between the teeth, gives flexibility to the archwire, and allows horizontal control of the tooth positions. The horizontal component gives more flexibility and provides vertical control. It is 2.5 times the length of wire in ordinary archwires and provides a 10-fold reduction in the load-deflection rate. The use of MEAW requires completion of all leveling and alignment, elimination of all poorly positioned brackets, and constant use of vertical elastics on the anterior teeth. It was originally prescribed for brackets with .018-in slots and .016 × .022-in archwires, allowing more flexibility for intrusive forces.
This article shows a successful treatment result in a growing patient with an Angle Class III subdivision malocclusion and an anterior open bite.
Case report
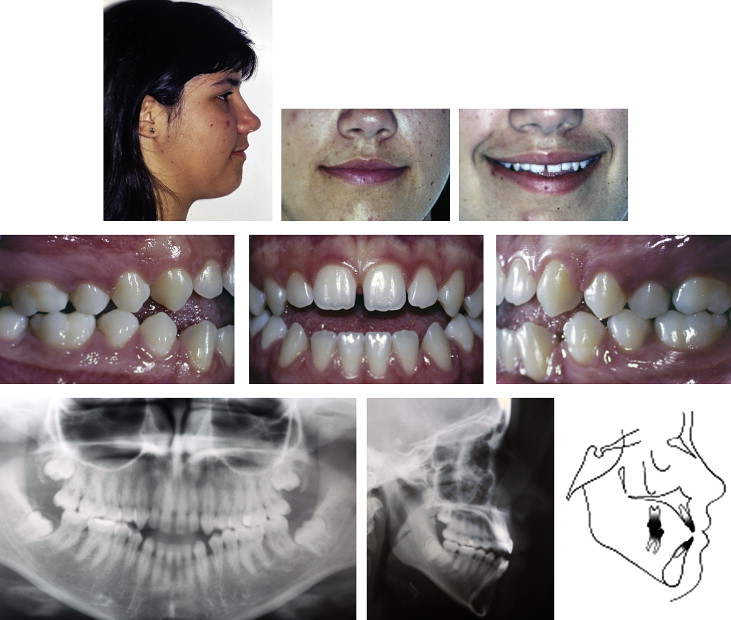
A girl, aged 14 years 8 months, was referred by her clinician to a private office after consulting 2 other orthodontists, with the complaint of an anterior open bite. She had a pleasant profile, although there was increased lower facial height and little incisor exposure during smiling ( Fig 1 ). She had an Angle Class III subdivision malocclusion, with an anterior open bite of 3.5 mm, an overjet of 0.5 mm, and a midline diastema. The mandibular dental midline was deviated to the left by 1.5 mm. Cephalometric analysis showed a skeletal Class I relationship (ANB angle, 4°) and a high mandibular plane angle (FMA, 32°). The maxillary incisors to NA angle was 19°; the maxillary incisors to NA distance was 4 mm; the anterior inferior teeth were protruded, with mandibular incisors to NB angle was 42°; and the mandibular incisors to NB distance wa 9 mm.
Several factors have been implicated as causes of an anterior open-bite malocclusion, including inherited facial form, unfavorable growth pattern, posture, sucking habits, nasopharyngeal airway obstruction, and tongue posture and function. Kim reported that the association of an inclined occlusal plane and mesial tipping of posterior teeth might cause an anterior open bite. In some cases, open bite is more likely to be produced by the interaction of different functional aspects and environmental influences with facial morphology. Our patient had a hyperdivergent facial profile but no history of sucking habits, mouth breathing, or abnormal tongue posture or swallowing.
The main objective of open-bite treatment in general is to achieve ideal overbite and overjet relationships. The vertical reference for anterior teeth would be the position of the maxillary central incisor relative to the inferior lip line. When treating an open-bite malocclusion, correction of the maxillary and mandibular occlusal planes and the axial inclinations of the teeth must be considered. Therefore, the orthodontist’s choice to intrude the molars or extrude the anterior teeth will be guided mainly by the vertical dimension of the lower face and the esthetic features of the anterior segment.
This patient’s Angle Class III malocclusion would be corrected by uprighting the mandibular posterior teeth and using intermaxillary elastics, with Class III resulting on the right side. A high-pull chincup would need to be worn 16 hours a day. Ideal overjet and overbite would be achieved by extruding the maxillary and mandibular anterior teeth, and also correcting the posterior tooth inclination, resulting in correction of the reverse curve of Spee in the mandibular arch. Because the patient had little maxillary central incisor exposure during smiling, the anterior tooth extrusion would also favor a more esthetic result. Delicate control of the facial height would be required.
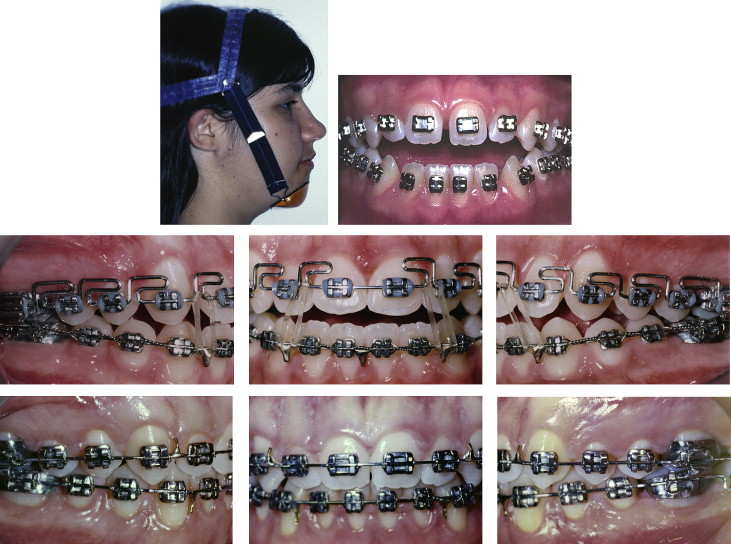
Full edgewise fixed appliances with 0.022-in slot brackets were placed. During the alignment and leveling stages, the patient wore a vertical chincup (16 hours a day) to prevent extrusion of the posterior teeth ( Fig 2 ). A .019 × .026-in stainless steel archwire, made with boot loops in all interproximal areas from the lateral incisors to the second molars, was used. On each loop, we checked lingual root torque, bilateral symmetry, and vertical-segment angulations to prevent gingival injuries. Tip-back bends were incorporated. The curve of Spee in the maxillary arch was increased and reversed in the mandible. The tip-back bends and the Spee curves provided intrusive forces on the maxillary and mandibular incisors, an effect opposed by 3/16-in elastics with vertical force placed in the canines’ mesial loops. These elastics delivered a 50-g force with the mouth closed and 150 g with moderate mouth opening.
After bite closure and finishing, the treatment objectives were achieved, and the appliances were removed ( Fig 3 ). Treatment time was 3 years. An Angle Class I molar relationship was achieved on both sides, and overjet, anterior open bite, and mandibular midline deviation were all corrected. As intended, the facial profile was maintained, and the incisors’ exposure during smiling increased.



