Introduction
Intraoral elastics are commonly used in orthodontics and require regular changing to be effective. Unfortunately, poor compliance with elastics is often encountered, especially in adolescents. Intention for an action and its implementation can be improved using “if-then” plans that spell out when, where, and how a set goal, such as elastic wear, can be put into action. Our aim was to determine the effect of if-then plans on compliance with elastics.
Methods
To identify common barriers to compliance with recommendations concerning elastic wear, semistructured interviews were carried out with 14 adolescent orthodontic patients wearing intraoral elastics full time. Emerging themes were used to develop if-then plans to improve compliance with elastic wear. A prospective pilot study assessed the effectiveness of if-then planning aimed at overcoming the identified barriers on compliance with elastic wear. Twelve participants were randomized equally into study and control groups; the study group received information about if-then planning. The participants were asked to collect used elastics, and counts of these were used to assess compliance.
Results
A wide range of motivational and volitional factors were described by the interviewed participants, including the perceived benefits of elastics, cues to remember, pain, eating, social situations, sports, loss of elastics, and breakages. Compliance with elastic wear was highly variable among patients. The study group returned more used elastics, suggesting increased compliance, but the difference was not significant.
Conclusions
The use of if-then plans might improve compliance with elastic wear when compared with routine clinical instructions.
The success of orthodontic treatment depends, in part, on patient compliance with advice, including diet, oral hygiene behaviors, maintenance of appliances, and adherence with adjuncts such as elastics. However, few studies have investigated the factors that predict compliance with elastic wear or tested interventions to improve compliance with this behavior. Egolf et al reported that compliance with elastics and headgear, as assessed by the clinician and by patient self-report, was correlated with psychological characteristics. Pain or dysfunction, health awareness, stoic or sensitive, and self-confidence and self-assurance characteristics had weak but significant correlations with compliance. When asked the main reason for not wearing headgear or elastics, the participants stated pain, laziness, forgetfulness, and embarrassment most frequently.
Orthodontists have adopted a variety of methods to improve compliance, including patient education, verbal praise, positive and negative reinforcement, charts, and rewards. Excellent communication and good rapport with patients are also important factors. The majority of these methods focus on changing the patients’ intentions to carry out the requested behavior because it is thought that this is the most immediate predictor of compliance. However, this assumes that people actually do what they intend. The gap between intended and actual behavior has been highlighted by Gollwitzer and Sheeran, who differentiated between an intention to engage in a behavior, “I want to do X,” and a plan to perform that behavior, “This is how I will do X.” This project focused on the latter process: the so-called implementation intentions. Implementation intentions are specific plans of action, usually identifying when, where, and how the person will engage in a specific behavior. These are formed as “if-then plans,” which state that “if Y occurs, then I will perform X.” Thus, they link the desired behavior to situational cues that trigger the behavior. They can also be used to identify what to do when a mistake is made or when a behavior has been forgotten.
The technique of if-then planning to change behavior has been tested in many fields, including education and health. A meta-analysis of 63 studies covering 94 independent interventions and 8461 participants published in 2006 found that if-then planning was effective in achieving behavioral change with a medium-to-large effect size (Somer’s d = 0.65). For health-related behaviors specifically, the review reported a medium effect size (d = 0.59) based on 23 studies involving 2861 participants. Only 3 studies have applied if-then planning in dentistry, all of which looked at flossing behaviors. Schuz et al found that planning was the only significant predictor of adherence to a daily regimen of flossing in 157 university dental students. Sniehotta et al developed a brief intervention to enhance intention implementation in a group of university students. By asking the participants to plan where and when they would floss their teeth, the authors were able to demonstrate an improvement in the proportion of those who were flossing 3 times a week or more. Similarly, Suresh et al found that keeping a flossing diary increased dental flossing and reduced plaque and bleeding scores in patients with periodontal disease in the short term.
The primary aim of this research was to pilot test the effectiveness of if-then planning on compliance with elastic wear. To achieve this, it was necessary to first identify common barriers to compliance with elastic wear, so the secondary aim was to investigate motivations for, and compliance with, elastic wear during orthodontic treatment.
Material and methods
Ethical approval was obtained from the National Research Ethics Service Committee London-East before the study. Informed consent was given by all participants before they entered the study, which comprised 2 parts as described below.
Part 1 was the qualitative phase. To identify the common barriers to compliance with elastic wear, semistructured interviews were carried out with 14 adolescent orthodontic patients who were recruited by their treating orthodontists during a routine visit to 1 of 2 district general hospital orthodontic departments in Aylesbury and Amersham, United Kingdom.
The inclusion criteria were patients (1) 10 to 16 years of age, (2) undergoing 2-arch fixed appliance treatment, (3) wearing Class II or Class III interarch elastics full time, and (4) able to consent (or having parental assent).
The exclusion criteria were patients (1) wearing extraoral elastics (eg, with headgear) or other types of intraoral elastics (eg, box elastics), and (2) with syndromes or clefts of the lip or palate or undergoing orthodontic treatment in conjunction with orthognathic surgery.
The participants comprised 9 girls (64%) and 5 boys (36%): 4 participants were 14 years old at the time of the interview, 2 were 15 years old, and 8 were 16 years old. Thirteen participants described their ethnicity as white British, and 1 was Asian.
The researchers, based on their clinical knowledge and the available research, developed a topic guide that was expanded as the interviewees raised new topics. All interviews were carried out by a trained interviewer who was also an orthodontist (H.J.V.).
The interviews were conducted away from the clinical setting and were recorded and then transcribed by the researchers. The interviews lasted from 5 minutes 44 seconds to 11 minutes 17 seconds; the average duration was 7 minutes 41 seconds. Although the topic guide was used as a framework for the interviews, the interviews were allowed to diverge into topics brought up by the participants when required, and any new themes were added to the topic guide for subsequent interviews. The interviews were carried out until no new themes were identified. The interview data were organized using a framework analysis that allowed themes and subthemes to be identified. An Excel spreadsheet (Excel 2010; Microsoft, Redmond, Wash) was used for organization and aided in the analysis of the large amount of information obtained.
The themes and subthemes identified from the interview data were used to develop an if-then planning scheme relevant to elastic wear, and this was incorporated into a leaflet that was used for the pilot study.
Part 2 was the pilot study of if-then planning. This was undertaken to determine the effect of if-then plans on compliance with elastic wear in a cohort of 12 adolescent patients.
The inclusion criteria were patients (1) 10 to 16 years of age, (2) undergoing 2-arch fixed appliance treatment, (3) commencing wearing Class II or Class III interarch elastics full time, and (4) able to consent (or having parental assent).
The exclusion criteria were patients (1) wearing extraoral elastics (eg, with headgear) or other types of intraoral elastics (eg, box elastics), and (2) with syndromes or clefts of the lip or palate or undergoing orthodontic treatment in conjunction with orthognathic surgery.
The participants were recruited between September 1, 2011, and December 31, 2011. Seven (58%) patients were girls, and 5 (42%) were boys. Eleven identified their ethnicity as white British, and 1 was Asian; all were medically fit and well. Their ages ranged from 13 to 16 years (3 participants were 13 years, 2 were 14 years, 2 were 15 years, and 5 were 16 years).
The participants were randomly allocated to either the intervention or the control group. The allocation sequence was determined using a random number table, and allocation concealment was achieved with opaque envelopes.
The study group (n = 6) received the if-then planning intervention, and the control group (n = 6) received the information routinely provided in the department when patients are asked to wear intraoral elastics. The delivery of the intervention and the instructions to both groups was done by a researcher (H.J.V.), and collection of the outcome data was undertaken by another author (H.C.T.). Although blinding was not possible at the intervention allocation, at data collection, the researcher was not aware of the participants’ group membership. Furthermore, statistical analysis was undertaken by a researcher (J.T.N.) who was masked to group membership.
To ensure standardization of the format for delivering the instructions for elastic wear, 2 DVDs were created: one for the study group and one for the control group. The participants were allowed to take this DVD home at the end of the appointment. One person (H.J.V.) delivered all instructions and interventions. All participants were given routine information about elastic wear that included the recommendation to put a new pair of elastics on twice a day, a demonstration of how to fit elastics, and information on the importance of elastic wear for their orthodontic treatment.
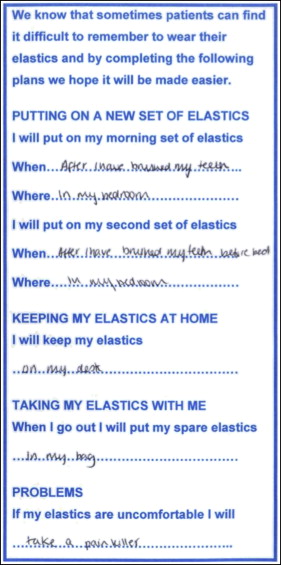
In addition, the participants in the intervention group were asked to formulate 4 if-then plans before leaving the appointment using a planning sheet designed on the basis of the information from the analysis of data from part 1 of the study, which asked the participants to identify (1) when and where to put on their new sets of elastics, (2) where to keep their elastics at home, (3) how to carry spare elastics with them when they went out, and (4) how to manage problems with elastics.
An example of a completed if-then planning sheet used in the study is shown in the Figure .
All participants were given 2 plastic bags, each containing an identical number of elastics (120 per bag). An additional empty resealable bag labeled “used elastics” was stapled to each bag of elastics. The instructions in the DVD asked participants to place all used elastics in this bag as they removed them from the mouth and to return both unused and used elastics at their next visit. A letter reminding participants to bring their used and unused elastics to their appointment was sent a week before the appointment. An assessment of compliance was made by counting the used and unused elastics. The number of elastics that would have been expected to be used was calculated based on the number of days between appointments, and compliance was calculated as a percentage of actual wear compared with ideal wear.
At the follow-up appointment, all participants were given a short questionnaire comprising 4 visual analog scales (10 cm) to assess their cognitions regarding the wearing of elastics, and their self-perceived compliance with elastic wear. Specifically, the participants were asked the following questions.
- 1.
How easy did you find it to remember to wear your elastics? (scale, 0-10 cm: very easy to very difficult)
- 2.
How easy was it to remember to always have your elastics with you? (scale, 0-10 cm: very easy to very difficult)
- 3.
In general, how easy was it to wear your elastics? (scale, 0-10 cm: very easy to very difficult)
- 4.
How many hours per day did you wear your elastics on average? (rating, 0-24 in units of 1 hour)
Statistical analysis
Descriptive statistics (medians, ranges) for all outcome measures were calculated. The proportion of elastics used as a function of the ideal and respondents’ self-reports of the cognitions and compliance regarding elastic wear were compared across the intervention and control groups using the Mann-Whitney U test.
Results
In part 1, the qualitative study, the analysis of the themes arising from the motivational and volitional factors described by the participants is summarized in Table I . Saturation was reached after 8 interviews, with no new themes emerging in subsequent interviews. The participants’ responses were classified into 3 broad categories: information on their orthodontic treatment; factors relating to their motivation (positive or negative intentions to wear their elastics); and most importantly for this study, volitional factors (factors that encouraged or inhibited the wearing of elastics).
| Orthodontic history and background information |
| Length of time in treatment |
| Length of time wearing elastics |
| Opinions on wearing fixed appliances |
| Friends’ experiences of orthodontics |
| Number of hours elastics worn |
| Frequency elastics changed |
| Motivational considerations |
| Perceived need |
| Perceived benefit |
| Perceived efficacy |
| Positives |
| Volitional considerations |
| Remembering |
| Internal cues |
| External visual cues |
| External direct cues/reminders |
| Availability |
| Storage/keeping |
| Losing elastics |
| Location/where they are at the time |
| Activties |
| Barriers |
| Forget |
| Discomfort |
| Restriction |
| Annoying/fed up |
| Difficulties putting in |
| Breakages |
| Esthetics |
| Social concerns/sports |
| Concerns regarding elastics |
| Eating |
| Lack of understanding of function |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


