Molar uprighting is an important adjunctive treatment in orthodontics: repositioning the tilted molar eliminates the potentially pathologic condition and simplifies the ultimate restorative procedure. Although various methods for molar uprighting have been applied successfully, they still have some limitations and disadvantages in tooth movement. This article reports on a new clinical technique for molar uprighting with nickel-titanium springs based on a setup model. Two patients treated with this system are shown.
A mesially tilted molar with a missing adjacent tooth is a common problem, and a number of approaches have been introduced for this clinical situation. Treatment modalities including various loop designs, tip-back springs with segmented arch systems, and open-coil springs with continuous archwire systems are widely applied with fixed orthodontic appliances. However, most of these devices exert a heavy force and cause unwanted movement of the adjacent teeth. In addition, the amount of tooth movement cannot be predicted with these devices. Here, we suggest an option for simple, accurate, and predictable molar uprighting.
Clinical applications
- 1.
In the initial model, the target tooth is set up in an ideal position in consideration of the relationship with the opposing teeth ( Fig 1 ).
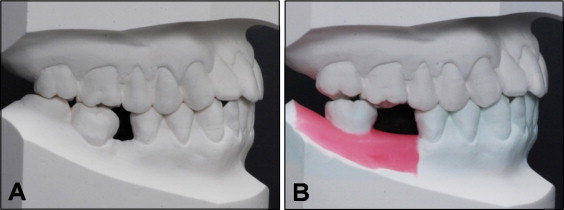
Fig 1 A, Initial model; B, ideal setup model. - 2.
The nickel-titanium spring is fabricated on this setup model. A round 0.014-in nickel-titanium sectioned wire is bonded passively to the model teeth with light-cured resin. This resin functions as a customized base ( Fig 2 ).
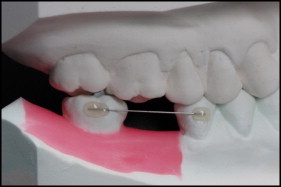
Fig 2 Fabrication of the nickel-titanium spring with a customized resin base. - 3.
The transferring jig for the nickel-titanium spring is built up with the light-cured blue resin, covers the whole customized resin base, and extends to the occlusal surface of the model teeth for a reference structure ( Fig 3 ).

Fig 3 Fabrication of the transferring resin jig for the nickel-titanium spring with a customized resin base. - 4.
The transferring jig with this nickel-titanium spring is separated carefully from the setup model. Next, the surface of the customized resin base is etched with an aluminum oxide microetcher (Microetcher II; Danville Materials, San Ramon, Calif).
- 5.
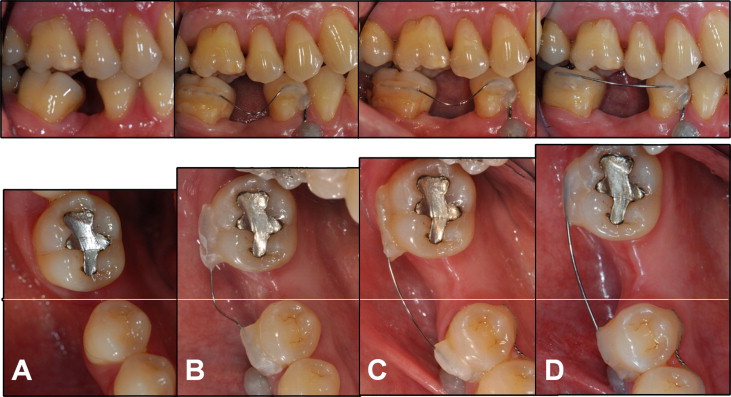
The buccal surfaces of the teeth are etched, rinsed, dried, and primed. The adhesive is applied to the customized resin base before positioning on the target teeth. The nickel-titanium spring is applied precisely to the planned position with the transferring resin jig. It is applied first to the tilted molar and light cured, and then to the premolar and light cured ( Fig 4 ). Afterward, the transferring jig is removed by a low-speed carbide bur.

Fig 4 Precise application of the nickel-titanium spring with a customized resin base through transfer of the resin jig. - 6.
The sequential nickel-titanium springs with larger diameters that were fabricated on same setup model can be applied.
Case reports
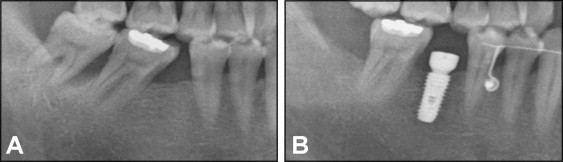
Patient 1 was a 45-year-old man with the chief complaint of a mesially tilted mandibular right second molar and a missing mandibular right first molar ( Fig 5 , A ).
An orthodontic mini-implant (diameter, 1.4 mm; length, 6 mm; Jeil Medical, Seoul, Korea) was inserted between the roots of the first and second premolars and was attached to the mandibular right second premolar with a 0.019 × 0.025-in stainless steel sectioned wire and resin for indirect skeletal anchorage.
The mandibular right third molar was extracted as planned, and then the 0.014-in nickel-titanium spring derived from the setup with the customized resin base was transferred to the mandibular right second molar and second premolar by the transferring system ( Fig 5 , B and C ).
After 8 months of treatment, the tilted second molar was successfully uprighted, and a 4.5-mm space was regained without extrusion or rotation of the molar. Moreover, no unwanted movement of the second premolar occurred because of the indirect skeletal anchorage. The orthodontic treatment was completed with passive bonding of the 0.016-in nickel-titanium sectioned wire on the mandibular right second molar and second premolar as a fixed retainer, and an implant prosthesis was placed in the first molar area ( Figs 5 , D , 6 , and 7 ). This outcome was performed by 1 nickel-titanium spring without reactivation or changing of the wire.