
Fig. 8.1
Three areas of missing posterior teeth. (a) Missing maxillary first molar. (b) Missing mandibular first molar. (c) Closure of E (deciduous second molar) space (mandible) when the permanent second bicuspid is missing
(iii)
Closure of E (deciduous second molar) space (mandible) (Fig. 8.1c) when the permanent second bicuspid is missing
2.
By the amount of mesial movement of the posterior teeth
(i)
Pure retraction of anterior teeth: In practice, there are very few cases of pure retraction of anterior teeth because the mesiodistal length of the first molar is very long.
(ii)
Reciprocal traction (Fig. 8.2a): Many cases fall under this category.
Fig. 8.2
(a) Reciprocal traction. (b) Pure protraction of the posterior teeth
(iii)
Pure protraction of posterior teeth (Fig. 8.2b): The missing first molar space is closed by pure protraction of the posterior teeth. If the first molar were intact, these cases could be treated by non-extraction. This is the most difficult type of teeth movement because the distance to be moved is the longest.
8.2 Cases of Molar Protraction
1.
Missing maxillary first molar (Fig. 8.3)
Fig. 8.3
(a) Initial, (b) during treatment, (c) debonding, (d) 1 year 8 months after debonding, (e) X-ray. A 20-year, 7-month-old female patient came for the correction of lip protrusion and crowding. Her maxillary left first molar was in a root rest state due to severe caries; therefore, the first molar was extracted instead of the bicuspid of the maxillary left side. At debonding, the missing first molar space closed completely. The lip protrusion and crowding improved. At 1 year and 8 months after debonding, there was no space relapse. The second and third molars looked like the first and second molars
2.
Missing mandibular first molar (Fig. 8.4)
Fig. 8.4
(a) Initial, (b) during treatment, (c) debonding, (d) 5 years and 8 months after treatment, (e) X-ray. A 16-year, 11-month-old female patient came for the correction of anterior crowding and protrusion. Her mandibular left first molar was severely damaged by caries. The first molar was extracted at that site, and on the other side, three bicuspids were extracted. The long distance of the mandibular left first molar extraction space was closed successfully. There was no space relapse 5 years and 8 months after debonding, despite no usage of a fixed wire retainer. The impacted third molar erupted well even though the configuration was not good. It will be usable for a considerable amount of time without major problems
3.
Closure of E (deciduous second molar) space (mandible) when permanent second bicuspid is missing (Figs. 8.5, 8.6 and 8.7)
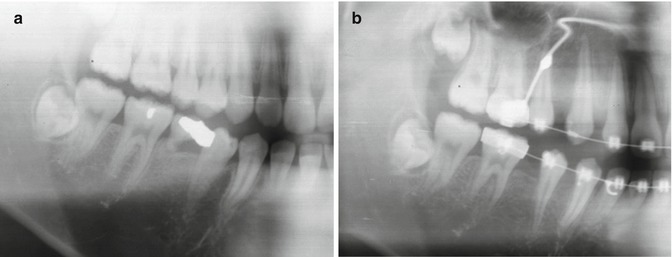
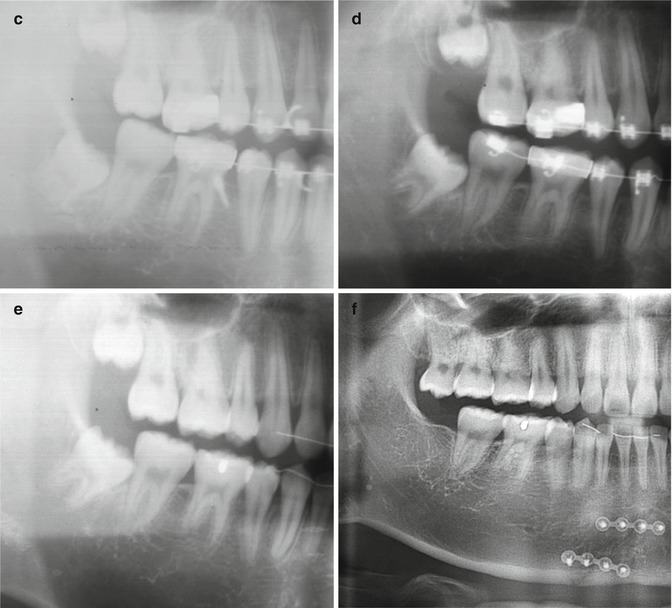
Fig. 8.5
(a) Initial, (b, c) during treatment, (d) debonding, (e) 4 years and 9 months after treatment. A 15-year, 11-month-old male patient came for the correction of anterior protrusion. The mandibular left and right second deciduous molars were retained and their successors (second bicuspids) were missing. Those teeth and the maxillary right and left first bicuspids were extracted. At debonding, bilateral Class I molar and canine relation had been achieved. The retraction of the anterior teeth reduced the protrusion of the lips. At 4 years and 9 months after treatment, stable occlusion and good function could be seen and there was no space relapse
Fig. 8.6
(Continued) Right side. (a) Initial, (b–d) during treatment, (e) debonding, (f) 4 years and 9 months after treatment
Fig. 8.7
(Continued) Left side. (a) Initial, (b, c) during treatment, (d) right before debonding, (e) 4 years and 9 months after treatment. Because of Leeway space, the mesiodistal length of the mandibular second deciduous molar was longer than that of its successors (second bicuspid). At debonding, the root arranged parallelly. The impacted mandibular third molar erupted successfully. His mandible was fractured 2 months before the follow-up and was operated on
8.3 Formation of Molar and Canine Relation
In this chapter, the term “Class I molar relationship” is used to specify the position of the second molars moved into the first molar location.
1.
Class I molar and Class I canine relation
(i)
Missing maxillary first molar and mandibular non-extraction (Fig. 8.8a)
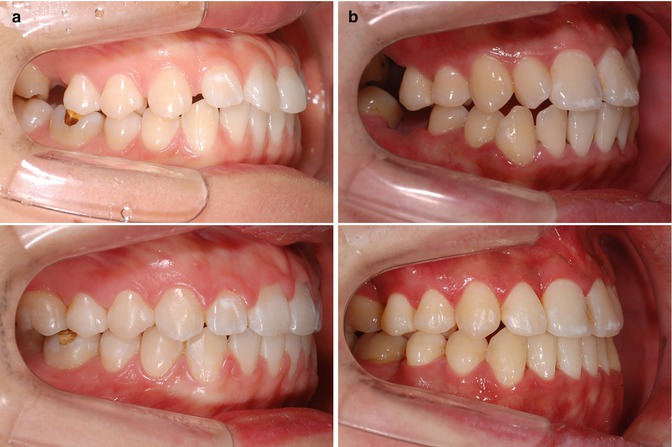

Fig. 8.8
Class I molar and Class I canine relation. (a) Missing maxillary first molar and mandibular non-extraction. (a–1) Before treatment. (a–2) After treatment. (b) Missing maxillary and mandibular first molar. (b–1) Before treatment. (b–2) After treatment. (c) Maxillary non-extraction and missing mandibular first molar. (c–1) Before treatment. (c–2) After treatment
2.
Class II molar and Class I canine relation
(i)
Maxillary bicuspid extraction and missing mandibular first molar (Fig. 8.9)
Fig. 8.9
Class II molar and Class I canine relation: maxillary bicuspid extraction and missing mandibular first molar. (a) Before treatment. (b) After treatment
3.
Class III molar and Class I canine relation
(i)
Missing maxillary first molar and mandibular bicuspid extraction (Fig. 8.10)
Fig. 8.10
Class III molar and Class I canine relation: missing maxillary first molar and mandibular bicuspid extraction. (a) Before treatment. (b) After treatment
8.4 Possible Problems and Biomechanics
8.4.1 Tipping of Adjacent Teeth
This 33-year-old female had been referred by other clinic (Fig. 8.11a, b). Her chief complaint was protrusion and she had a bad mandibular left first molar. Three bicuspids and the mandibular first molar had been extracted with the space closed at the previous clinic. At this stage (Fig. 8.11c), when she came to my clinic, the second molar showed severe tilting. Within 4 years and 6 months after the start of treatment, the periodontium had been severely damaged. The root barely moved. This is the most common complication of this treatment.
Fig. 8.11
(a) Initial, (b) during treatment, (c) 4 years 6 months after the start of treatment
8.4.2 Mesial Rotation and Buccal Sweeping
When protracting the second molars, mesial rotation and swinging into the buccal side of the protracted second molars may occur, which can create a posterior crossbite (Fig. 8.12). To prevent this, a rigid lingual arch and a lingually placed TSAD can be used. However, the lingual arch may not only cause discomfort to the patient but also interfere with further mesial movement. In addition, the lingual arch needs to be remade when it touches the lingual side of the anterior teeth. Lingual placement of the TSAD is very difficult because of poor vision and accessibility. Other methods are placing an elastic chain from the lingual side of the molars to a button on the canine or a sliding band with a lingual arch. In the cases in this book, this problem was minimized by inserting an anti-rotation bend in the posterior portion of the arch wire.
Fig. 8.12
Protraction force (B) produced buccal force (A). This swung the posterior dentition into a unilateral crossbite
8.4.3 Extrusion of the Posterior Teeth
During the protraction, the extrusion of the posterior teeth caused an anterior open bite (Fig. 8.13). The entire arch rotates around the center of rotation of the whole dentition in the TSAD retraction system (Fig. 8.14). As a result, when the posterior teeth were protracted, the molars are extruded, causing an anterior open bite.
Fig. 8.13
Bite opening during molar protraction (a) initial, (b) during molar protraction, (c) open bite worsened
Fig. 8.14
The center of rotation of the entire arch (a) is located under the TSAD (red point). Protraction of the posterior teeth caused the extrusion of the posterior tooth (b) and intrusion of the anterior teeth (c)
To solve these problems, the following methods are suggested: (1) A long hook can be attached to the second molar brackets to relocate the protracting force near the center of rotation. (2) The maxillary and mandibular molar intrusion can be done by TSAD.
8.5 Other Cases
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


