Introduction
The aim of this study was to evaluate the density of the midpalatal suture as assessed by low-dose computed tomography (CT) before rapid maxillary expansion (RME) (T0), at the end of active expansion (T1), and after a retention period of 6 months (T2).
Methods
The study sample comprised 17 prepubertal subjects (mean age, 11.2 years) with constricted maxillary arches and unilateral or bilateral posterior crossbite. The total amount of expansion was 7 mm in all subjects. Multi-slice low-dose CT scans were taken at T0, T1, and T2. On axial CT scanned images, 4 regions of interest (ROIs) were placed along the midpalatal suture (anterior [AS ROI] and posterior [PS ROI]) and in 2 regions of palatal bone (anterior and posterior). Density was measured in Hounsfield units. The Mann-Whitney U test and Friedman analysis of variance (ANOVA) with post-hoc test were used ( P <0.05).
Results
The densities in the AS and PS ROIs were significantly smaller than the reference bone densities before RME therapy. Both AS and PS ROIs showed significant decreases in density from T0 to T1, significant increases from T1 to T2, and no significant differences from T0 to T2.
Conclusions
The effective opening of the midpalatal suture by RME in prepubertal subjects was associated with a significant decrease in sutural density. The sutural density after 6 months of retention post-RME indicated reorganization of the midpalatal suture, since it showed values similar to the pretreatment ones.
Rapid maxillary expansion (RME) is an effective orthopedic procedure commonly used to treat maxillary transverse deficiencies in growing patients. Transverse dentoskeletal changes in the maxilla in response to RME are produced mainly through disruption of the midpalatal suture. Histologic studies on both humans and animals supported the opening of the midpalatal suture after RME therapy. In a study of 6 monkeys, Cleall et al reported that, at the moment of suture opening, the area was filled with unorganized fibrous conjunctive tissue; 6 months after expansion, the suture was well organized and appeared histologically normal.
Dimensional changes in the midpalatal suture produced by RME in growing subjects have been investigated by conventional radiographic techniques such as posteroanterior cephalograms and occlusal radiographs. Recently, the opening of the midpalatal suture after RME was evaluated with computed tomography (CT), which provides accurate 3-dimensional assessment of skeletal changes. The use of CT has been proposed also for the quantitative evaluation of bone density with the Hounsfield index in selected regions of interest (ROI). The same index has been used to assess bone density for implant placement in the maxillary bones.
The aim of this study was to evaluate treatment and posttreatment changes produced by RME in the density of the midpalatal suture with a low-dose CT protocol.
Material and methods
The prospective study sample comprised 17 white subjects (7 boys, 10 girls) with a mean age of 11.2 years (range, 8-14 years) who sought orthodontic treatment at the Department of Orthodontics of the University of Rome “Tor Vergata.” Criteria for enrollment in the study were as follows: constricted maxillary arches with or without unilateral or bilateral posterior crossbite, and prepubertal stages of cervical vertebral maturation (CS1-CS3) as assessed on lateral cephalograms. This project was approved by the ethical committee, and informed consent was obtained from the patients’parents.
Each patient underwent a standardized protocol of RME with the butterfly palatal expander that followed the basic design of Haas. The expansion screw was activated twice per day (0.25 mm per turn) for 14 days, for a total amount of screw expansion of 7 mm in all subjects. Then the screw was tied off with a ligature wire, and the expander was kept in place as a passive retainer for 6 months.
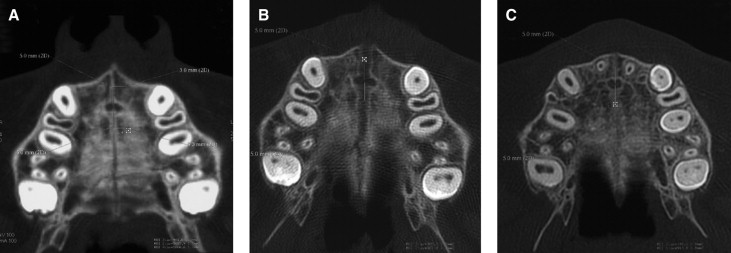
Multi-slice low-dose CT scans were taken before rapid palatal expansion (T0), at the end of the active expansion phase (T1), and after the retention period of 6 months (T2). The low-dose CT scan protocol was described previously. Standardized axial CT images parallel to the palatal plane and passing through trifurcation of the maxillary right first molar were acquired and enlarged by a 3-times magnification factor with specific software (Light-Speed 16, General Electric Medical System, Milwaukee, Wis). On the enlarged images, 4 ROIs that extended to an area of 1 mm 2 were placed by 1 trained operator (R.L.) for the calculation of values of density in Hounsfield units (HU) ( Fig ). The operator was blinded to the patient being measured. The 4 ROIs in the palatal region were defined as follows.
- 1.
Anterior sutural ROI (AS ROI): density values measured in the ROI located along the midpalatal suture 5 mm in front of the center of the nasopalatine duct at T0, T1, and T2.
- 2.
Posterior sutural ROI (PS ROI): density values measured in the ROI located along midpalatal suture 5 mm posterior to the center of the nasopalatine duct at T0, T1, and T2.
- 3.
Anterior bony ROI (AB ROI): density values measured in the ROI located on the palatal bone 3 mm laterally (on the right side) to the AS ROI at T0.
- 4.
Posterior bony ROI (PB ROI): density values measured in the ROI located on the palatal bone 3 mm laterally (on the right side) to the PS ROI at T0.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


