A mini dental implant (MDI) has a diameter ranging from 1.8 to 2.4 mm, whereas an implant with a diameter of 2.75 to 3.25 mm is referred to as a small diameter implant (SDI). The smallest conventional implant measures 3.25 mm. For the purposes of this chapter, all implants with a diameter of less than or equal to 3.25 mm will be referred to as miniimplants. For comparison, Figure 35-1 shows three Entegra implants of decreasing diameter and an INTRA-LOCK miniimplant of 2 mm in diameter ( Figure 35-1 ).

Miniimplants were initially used as transitional implants to support overdentures during phase 1 of conventional implant placement. The miniimplants were temporarily placed between conventional implants, allowing them to osseointegrate while the miniimplants bore the load of the dentures ( Figure 35-2 A, B ); however, when the time arrived to remove the temporary miniimplant, the practitioner often found it had integrated with the bone and was difficult to remove. Balkin reports two cases where miniimplants were used as transitional implants and later explanted and found to be osseointegrated when studied under light microscopy. Although miniimplants are still used for transitional purposes, many manufacturers are now approved by the Food and Drug Administration to market their product for long-term use. Various modifications and implant head morphologies have been developed to increase the versatility of the miniimplant. Current uses now include:
- •
Prosthodontic applications
- •
Stabilization of complete dentures
- •
Stabilization of removable partial dentures (RPDs)
- •
Pontic support of a fixed partial denture (FPD)
- •
Retention of obturators
- •
Single-tooth implant restorations in narrow spaces
- •
Orthodontic anchorage

▪
STABILIZATION OF COMPLETE DENTURES
Achieving stability of dentures has been a major challenge for prosthodontists and general dentists when making dental prostheses for patients with atrophic alveolar ridges. These patients complain of difficulty talking and eating as a result of poor retention of their dentures. Miniimplants with an o-ring attachment may be placed transmucosally beneath an existing full denture, and the denture may be retrofitted, or a new denture can be fabricated with o-ring receptors to engage the implants, affording patients added stability and retention of their denture ( Figure 35-3 A-D ). Griffitts conducted a study in which 100% of subjects who returned a questionnaire 5 months after receiving miniimplants under their existing denture reported dramatic improvements in comfort, retention, chewing ability, and speaking ability.
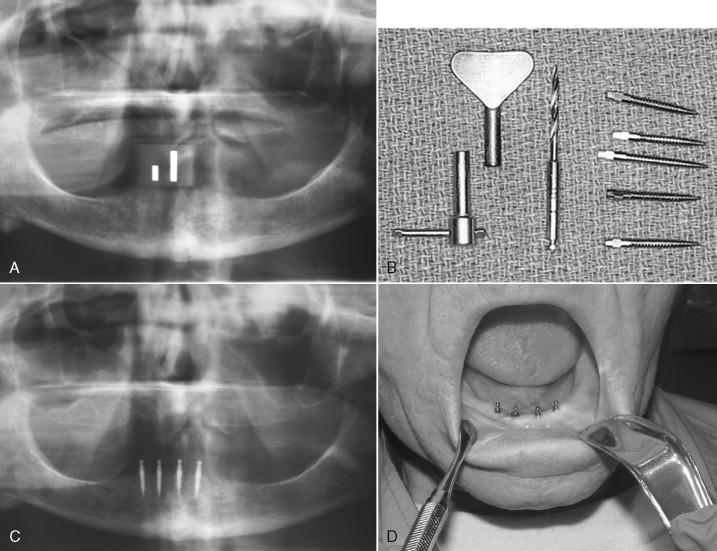
Miniimplants also contribute to patient satisfaction as a result of their relatively simple placement and ability to be immediately loaded after placement. A gingivoperiosteal flap is not necessary to place a miniimplant. The Imtec website recommends that the site of placement simply be marked with ink or with a bleeding point created by the tip of the pilot bur before making the pilot hole transgingivally. Ahn recommends that the pilot hole only be drilled one-half the length of the miniimplant, thus allowing the implant to provide primary mechanical retention immediately after placement. If primary stability is achieved, the miniimplants may be immediately loaded, allowing the patient to avoid an awkward edentulous phase, which is sometimes required while conventional implants osseointegrate. The Imtec Web page describes the surgical protocol for placing MDI miniimplants and states that the primary reason for not achieving adequate primary stability and nonintegration is overinstrumentation of the bone. If no significant resistance is encountered while advancing the miniimplant, overinstrumentation may have occurred or the bone may lack the required density, and the prognosis for the miniimplant reaching its full potential is doubtful. If adequate primary stability is encountered while placing the miniimplant, the long-term prognosis of the implant after immediate loading is improved.
Bone density is a major determining factor of the primary stability and success of miniimplants. The highest success rate is found in the dense bone of the anterior mandible with lower rates in the maxilla. When placing a miniimplant in very dense bone, it has been suggested that upon encountering resistance the implant be unscrewed one-half to one full turn and then advanced again. This process may need to be repeated multiple times, but will decrease the risk of implant fracture during placement. The use of titanium alloy implants rather than pure titanium may also decrease the risk of implant fracture during placement.
If you are placing miniimplants for transitional purposes, it has been suggested that the implant be placed at least 2 mm from the intended long-term implant to prevent bone resorption.
Miniimplants are an excellent solution to provide stability to dentures for transitional purposes and for long-term use. When placed using proper technique, they provide immediate stability and contribute to patient satisfaction aesthetically, functionally, and financially.
▪
STABILIZATION OF REMOVABLE PARTIAL DENTURES
Christensen suggests that miniimplants are an excellent way to improve patient satisfaction for those who wear a removable partial denture. In situations where there are bilateral distal extensions (Kennedy class I), unilateral distal extensions (Kennedy class II), or an anterior edentulous extension (Kennedy class IV), a miniimplant may be recommended to a patient to improve retention and decrease rocking of the RPD toward the edentulous span. Placement of the miniimplant in this situation is similar to placement under a full denture and will require that the denture be retrofitted to engage the miniimplant.
▪
STABILIZATION OF REMOVABLE PARTIAL DENTURES
Christensen suggests that miniimplants are an excellent way to improve patient satisfaction for those who wear a removable partial denture. In situations where there are bilateral distal extensions (Kennedy class I), unilateral distal extensions (Kennedy class II), or an anterior edentulous extension (Kennedy class IV), a miniimplant may be recommended to a patient to improve retention and decrease rocking of the RPD toward the edentulous span. Placement of the miniimplant in this situation is similar to placement under a full denture and will require that the denture be retrofitted to engage the miniimplant.
▪
PONTIC SUPPORT OF A FIXED PARTIAL DENTURE
If a bridge has become dislodged from one of its abutments and may be removed from the other abutment without damage, it is possible to salvage the bridge by recementing the bridge to its abutments after placing a miniimplant under the pontic for supplemental retention. This manner of salvaging an FPD will be agreeable to a financially concerned patient because a miniimplant is much less expensive than remaking a bridge. Patient satisfaction is improved because the bridge may be cemented the same day the implant is placed.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


