37 Metastases to the Major Salivary Glands from Non–Head and Neck Primary Malignancies
Metastases to the Parotid Gland
Metastases to the Submandibular Gland
Introduction
Metastases to the major salivary glands come from either supraclavicular or infraclavicular primary sites. The parotid gland is the major salivary gland most frequently involved by metastatic disease (80%–90%). By far the most common metastases to the parotid gland are from head and neck cutaneous squamous cell carcinomas and melanomas (see Chapter 36). This chapter concentrates on non–head and neck primary sites.
While supraclavicular sites metastasize via lymphatic spread or direct extension, infraclavicular sites spread predominantly via hematogenous routes. Consequently, metastases from infraclavicular sites tend to involve the salivary gland parenchyma more often, whereas head and neck primary sites often metastasize into the extraglandular and intraglandular lymph nodes (Figs. 37.1, 37.2, 37.3).1

Fig. 37.1 A 59-year-old woman who presented with a lump on the left parotid gland. The clinical appearance of the lump is suggestive of malignancy.
Metastases from infraclavicular primary sites are rare, with the literature consisting of case reports involving the parotid gland. The commonest primary sites are the lung, breast, and kidney, although metastases from the stomach, bladder, and prostate have also been described. Seifert et al.2 analyzed 108 cases of metastases to the salivary glands between 1965 and 1985. They found 21 cases from infraclavicular primary sites: seven from the lungs, six from the kidneys, six from the breast, one from the colon, and one from a uterine primary. Salivary gland metastases may be the presenting finding in patients with an asymptomatic infraclavicular primary neoplasm, or they may appear in patients with a known malignancy, sometimes many years after initial diagnosis of the primary.
 Metastases to the major salivary glands are most commonly of head and neck origin. Metastases from infraclavicular sites are rare, with the lung, kidney, or breast being the most likely primary site. By far the most frequently affected gland is the parotid.
Metastases to the major salivary glands are most commonly of head and neck origin. Metastases from infraclavicular sites are rare, with the lung, kidney, or breast being the most likely primary site. By far the most frequently affected gland is the parotid.
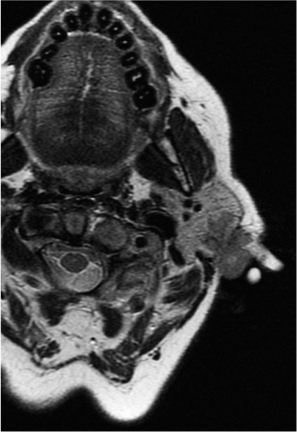
Fig. 37.2 An axial T2-weighted fast relaxation fast spin echo (FRFSE) sequence magnetic resonance scan in the same patient, showing the superficial location of the lump, with limited involvement of the parenchyma of the parotid gland.
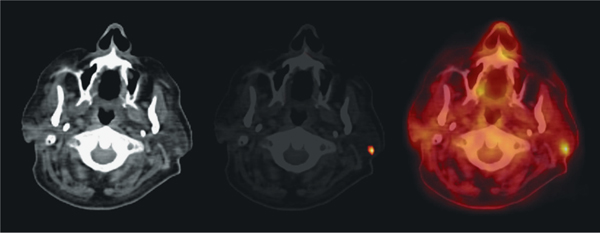
Fig. 37.3 Computed tomography (CT, left), fluorine F 18 fluorobolic activity within the lump in the left parotid, with a standard updeoxyglucose (FDG) positron-emission tomography (PET, center), take value of 7.8. A primary was found in the lung in this patient. and FDG PET–CT fusion scan (right) in this patient, confirming meta-
Metastases to the Parotid Gland
 From Lung Carcinoma
From Lung Carcinoma
Imauchi et al.3 report the case of a patient who presented with a parotid lump, which was demonstrated on computed tomography (CT) and magnetic resonance imaging (MRI). The fine-needle aspiration (FNA) biopsy showed an adenocarcinoma, and the patient underwent a total parotidectomy and modified radical neck dissection. Interestingly, the pathology showed parotid and cervical lymph-node involvement, with the parotid parenchyma spared. Although an initial chest radiograph was clear, a subsequent postoperative CT of the chest revealed the primary within the lung, in association with vertebral metastases. In the absence of facial nerve palsy, malignant FNA result, or clinical cervical lymphadenopathy, many clinicians would request either an ultrasound, CT, or MRI of a primary salivary gland lesion. The finding of adenocarcinoma on FNA indicates a need to include the neck, chest, and abdomen in the imaging examinations. A CT scan or co-registered CT–positron emission tomography (CT–PET) would therefore be recommended in order to locate any possible primary lesion.
 Patients with FNA of a parotid mass that shows adenocarcinoma or clear cells should be investigated with imaging to cover the neck, chest, and upper abdomen to ensure that primary sites are not overlooked.
Patients with FNA of a parotid mass that shows adenocarcinoma or clear cells should be investigated with imaging to cover the neck, chest, and upper abdomen to ensure that primary sites are not overlooked.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


