Fig. 4.1
The trigeminal nerve distribution
-
Hyperalgesia due to inflamed nerves and lowered thresholds (Byers et al. 1990).
-
Low pH of infected/inflamed tissues reduces the amount of uncharged basic form to penetrate nerve bundle.
-
Operator error: missing the block.
-
Tetrodotoxin-resistant (TTX-R) sodium channels which are resistant to local anesthetics (LA) (increased expression in symptomatic irreversible pulpitis (SIP) cases).
-
Apprehensive patients have decreased pain thresholds.
-
Acute tachyphylaxis: depletion of available neurotransmitters or receptors (Hargreaves 2003).
Management of local anesthetic failures:
-
Provide supplemental local anesthesia:
-
Block the population of tetrodotoxin-resistant (TTX-R) sodium channels that may be elevated in the inflamed state (Novakovic et al. 1998).
-
Aim higher on the 2nd IAN block: Gow–Gates or Vazirani–Akinosi (closed mouth mandibular block) (Fig. 4.3a, b).
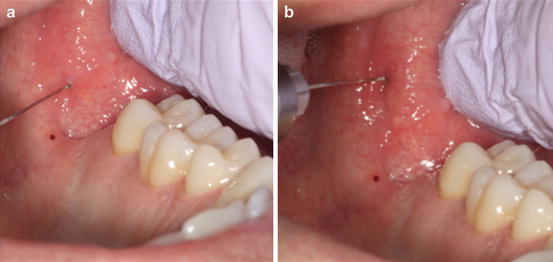 Fig. 4.3(a) Inferior alveolar block and (b) aiming higher on the 2nd inferior alveolar block
Fig. 4.3(a) Inferior alveolar block and (b) aiming higher on the 2nd inferior alveolar block -
Mental nerve block: The mental foramen can also be located via palpation, periapical radiographs, and panoramic radiographs (Aminoshariae et al. 2014). Additionally, the average location of the mental foramen is 60 % of the distance from the tip of the buccal cusp of the mandibular 2nd premolar to the inferior border of the mandible (Phillips et al. 1990).
-
Use an anesthetic with a lower pKa 3% mepivacaine since it decreases the potential for ion trapping, increases the concentration of local anesthetic molecules in their base form, and increases diffusion of the LA across nerve terminals, thus increasing onset of anesthesia.
-
Adjunctive injections: intraligamentary, intraosseous (IO), intrapulpal (see descriptions below in Section 2).
-
Adjunctive drugs: fast-acting nonsteroidal anti-inflammatory drugs (NSAIDs). Ibuprofen in a liquid gel form reduces levels of inflammatory mediator prostaglandin E2 (PGE2); this is a hypothesis and has not been evaluated in endodontic patients.
-
Anxious patients may benefit from nitrous oxide prior to giving any type of injection. Additionally, anxiolytic therapy my also be provided for the patient prior to their dental appointment. These medications are both safe and effective for dental outpatients. Studies have shown that triazolam (0.25 mg) can be an effective anxiolytic than diazepam (5.0 mg) for endodontic patients (Erich et al. 1997). Provide the patient with a prescription for two tablets of triazolam (0.25 mg), have the patient take one, one hour before their dental appointment, and instruct them to bring the remaining tablet with them to their dental appointment. Side effects include dizziness, drowsiness, and loss of coordination, thus the patient must have a driver accompany them to and from their dental appointment.
-
Distraction techniques such as jiggling the patient’s lip or quickly pulling the soft tissue over a stationary needle tip may aide in anesthetizing the anxious patient.
4.2 Techniques for Delivery of Anesthesia
- A.
Mandibular block:If the initial block does not anesthetize a patient after 10 min, a second block should be attempted at a higher angle as the mandibular foramen may be positioned higher.
- B.
Infiltration:
-
Supplemental buccal and lingual infiltrations of 4 % articaine or 2 % lidocaine increase the success rate of IAN block in patients with symptomatic irreversible pulpitis (SIP) (Aggarwal et al. 2009).
-
- C.
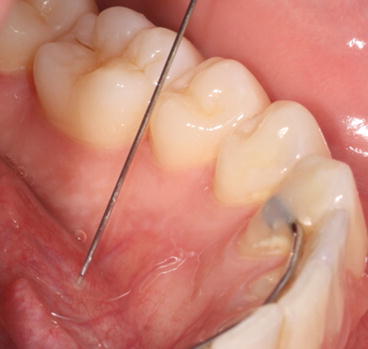
Intraosseous (IO): Delivers a local anesthetic solution directly into the cancellous bone adjacent to the tooth to be anesthetized. Given once signs of lip numbness have developed (Hargreaves 2010) (Fig. 4.4).
 Fig. 4.4Intraosseous anesthesia needle position
Fig. 4.4Intraosseous anesthesia needle position-
The two IO systems that have been researched include the Stabident system (Fairfax Dental Inc, Miami, FL) and X-tip (Dentsply, Tulsa, OK). Both IO, systems demonstrated similar success onset, duration, and perceived heart rate increases (Gallatin et al. 2003) (Fig. 4.5).
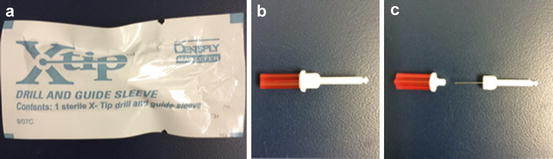 Fig. 4.5Intraosseous anesthesia: X-tip. (a) package; (b) guide sleeve (inside red cap); (c) drill
Fig. 4.5Intraosseous anesthesia: X-tip. (a) package; (b) guide sleeve (inside red cap); (c) drill -
Research has demonstrated that 67 % of patients had an increase in heart rate with an IO injection. No contraindications with healthy patients, but consider using an anesthetic without epinephrine, such as 3 % mepivacaine.
-
Stabident with 2 % lidocaine was shown to be 88 % effective for patients experiencing SIP.
-
Stabident with 3 % mepivacaine for SIP was 80 % successful with one injection and 98 % with two injections (Nusstein et al. 1998).

Stay updated, free dental videos. Join our Telegram channel

VIDEdental - Online dental courses


-
