Introduction
The aim of this study was to determine the effects of the leveling of the curve of Spee in subjects treated with preadjusted appliances in different skeletal vertical patterns.
Methods
The study sample consisted of 90 white patients (39 male, 51 female; age, 19 years 4 months ± 1 year 9 months), with a curve of Spee of 2 mm or greater before treatment. They were categorized into 3 groups: low-angle group (30 subjects; 12 male, 18 female; age, 19 years 1 month ± 1 year 4 months), normal-angle group (30 subjects; 14 male, 16 female; age, 19 years 6 months ± 2 years 1 month), and high-angle group (30 subjects; 13 male, 17 female; age, 19 years 7 months ± 1 year 5 months) by their vertical facial types. Cephalometric parameters were used to evaluate the different dental movements after treatment. The curve of Spee was measured on digital dental casts. Analysis of variance was used to determine any differences between the changes in the groups with time.
Results
For the skeletal variables, no significant modifications were found in the 3 groups. For the dentoalveolar variables, the low-angle group showed significant buccal movements and intrusion of the mandibular incisors. The high-angle group had greater extrusion of the posterior teeth associated with uprighting of the first and second molars.
Conclusions
In low-angle subjects, leveling of the curve of Spee occurs through buccal movement and intrusion of the mandibular incisors; in high-angle subjects, it occurs through extrusion and uprighting of the posterior teeth.
Highlights
- •
Leveling the curve of Spee in subjects with different skeletal vertical patterns was studied.
- •
For skeletal variables, no significant modifications were seen in the 3 groups.
- •
The low-angle group showed buccal movements and mandibular incisor intrusion.
- •
The high-angle group had greater posterior tooth extrusion and uprighting.
The curve of Spee is a naturally occurring phenomenon in the human dentition, and it is determined clinically by the distal marginal ridges of the posterior teeth in the arch and the incisal edges of the central incisors.
The development of curve of Spee probably results from a combination of different factors including differences in the times of eruption of the mandibular permanent teeth, variations in skeletal morphology and growth of orofacial structures, sagittal jaw relationship and incisor occlusion, and development of the neuromuscular system.
Andrews described the 6 characteristics of normal occlusion and found that the curve of Spee in subjects with good occlusion ranged from flat to mildly curved, noting that the best intercuspation occurred when the occlusal plane was relatively flat. He proposed that flattening the occlusal plane should be the treatment goal in orthodontics.
Various sophisticated approaches to level the curve of Spee were suggested by Burstone from true incisor intrusion to eruption of the posterior teeth without altering the positions of the incisors. At the same time, leveling with round cross-section archwires or rectangular cross-section archwires combined with torqued incisor brackets is clinically popular because of its simplicity. In either method, only 1 outcome occurs at the end of leveling: posterior elevation and proclination of the incisors (or masking by a cross-arch canine width increase).
Although leveling the curve of Spee is a common occurrence in orthodontic practices, few studies have been dedicated to examination of the relationship between orthodontic leveling of the curve of Spee and vertical skeletal pattern.
A simple correlation analysis between the radius or the depth of the curve of Spee and skeletal facial types was conducted. Farella et al reported, before orthodontic treatment, a weak association between the variation of the curve of Spee and the horizontal and vertical position of the mandible. Only 1 study has analyzed the variation of some morphologic characteristics with orthodontic treatment according to facial type and reported significant differences in overbite correction between low-angle and high-angle subjects after treatment.
However, no studies have analyzed whether vertical skeletal patterns influence orthodontic movements during leveling of the curve of Spee.
The aim of this study was to evaluate the treatment effects after leveling of the curve of Spee with full fixed edgewise preadjusted appliance in subjects with different skeletal vertical patterns.
Material and methods
The sample for this retrospective study consisted of 90 white patients’ orthodontic records (39 male, 51 female; mean age, 19 years 4 months ± 1 year 9 months) treated without extractions at the Department of Orthodontics at the University of Rome Tor Vergata in Italy. These patients were selected using the following inclusion criteria: full permanent dentition (excluding third molars, extracted or not erupted), curve of Spee 2 mm or greater before treatment, skeletal Class I (ANB angle, 0°-4°) or skeletal Class II (ANB angle, >4°) patterns (skeletal Class III were excluded because in these subjects the deph of curve of Spee results to be reduced before treatment ), postpubertal stage of skeletal maturity according to the cervical vertebral maturation method, no previous orthodontic treatment, no periodontal disease or morphologic tooth anomaly, no dental restoration or crown, and no mandibular asymmetry. All subjects were categorized based on Little’s irregularity index for anterior crowding as moderate irregularity.
Only patients with complete orthodontic records were selected for this study. The records consisted of dental casts and lateral cephalograms before treatment (T1) and after orthodontic therapy (T2). All subjects were treated with full fixed conventional preadjusted edgewise brackets with McLaughlin-Bennet-Trevisi values for tip and torque and a 0.022-in slot. A standard continuous archwire sequence (016-in round, 0.017 × 0.025-in rectangular, 0.019 × 0.025-in rectangular martensitic active nickel-titanium alloys [3M Unitek, Monrovia, Calif], and 0.019 × 0.025-in stainless steel) was used in all subjects. Alignment and leveling were considered obtained when passive engagement of a 0.019 × 0.025-in stainless steel archwire was achieved. The average duration of treatment was 24 ± 4 months. No auxiliary or curve of Spee wires were used during the treatment phases. All archwires used were of uniform arch form, and attachments were placed on all teeth from second molar to second molar.
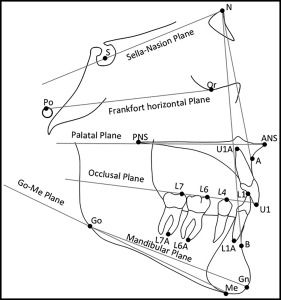
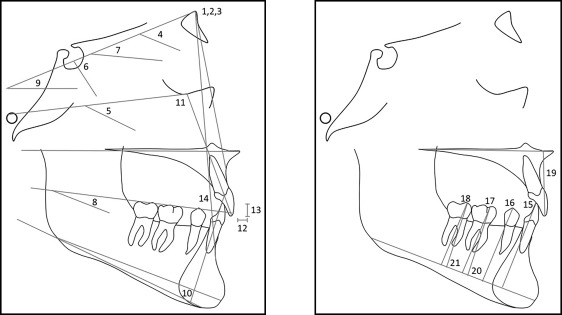
The cephalometric radiographs were scanned into imaging software (version 11.0; Dolphin Imaging, Chatsworth, Calif). Standard cephalometric landmarks were then identified on each radiograph; the functional occlusal plane (OP) was defined by a line intersecting the intercuspation of the posterior occlusion ; the palatal plane (PP) was defined by the ANS-PNS plane; the mandibular plane (MP) was defined by the Go-Gn plane. These cephalometric landmarks and reference planes are shown in Figure 1 . The following measurements were determined on each lateral cephalogram: SNA, SNB, ANB, SNˆGoGn, FMA, y-axis, SNˆOP, OPˆMP, SNˆPP, IMPA, Up.Inc.ˆFP, overjet, overbite, and interincisal angle (Int.Inc.). The cephalometric measurements used in this study are shown in Table I and Figure 2 .
| Measurement | Definition |
|---|---|
| Angular measurements (°) | |
| SNA | Angle between SN plane and NA plane |
| SNB | Angle between SN plane and NB plane |
| ANB | Difference between SNA and SNB |
| SNˆGoGn | Angle between SN plane and mandibular plane |
| FMA | Angle between FP plane and Go-Me plane |
| y-axis | Angle between FP plane and line of S-Gn |
| SNˆOP | Angle between SN plane and occlusal plane |
| OPˆMP | Angle between occlusal plane and mandibular plane |
| SNˆPP | Angle between SN plane and palatal plane |
| IMPA | Angle between mandibular plane and line of L1-L1A |
| Up.Inc. ˆFP | Angle between FP plane and line of U1-U1A |
| Int.Inc. | Angle between line of U1-U1A and line of L1-L1A |
| L6ˆMP | Angle between mandibular plane and line of L6-L6A |
| L7ˆMP | Angle between mandibular plane and line of L7-L7A |
| Linear measurements (mm) | |
| Overjet | Sagittal linear distance from L1 to U1 |
| Overbite | Vertical linear distance from L1 to U1 |
| L1-MP | Linear distance from L1 to mandibular plane |
| L4-MP | Linear distance from L4 to mandibular plane |
| L6-MP | Linear distance from L6 to mandibular plane |
| L7-MP | Linear distance from L7 to mandibular plane |
| U1-PP | Linear distance from U1 to palatal plane |
After data collection, the subjects were grouped according to their facial types (normal angle, high angle, low angle) based on their pretreatment cephalometric values for y-axis, mandibular plane angle, and SNˆGoGn angle. The normal-angle group (30 subjects; 14 male, 16 female; mean age, 19 years 6 months ± 2 years 1 month) included subjects with a mandibular plane angle between 23° and 28°, y-axis between 63° and 69°, and SNˆGoGn angle between 27° and 37°. The high-angle group (30 subjects; 13 male, 17 female; mean age, 19 years 7 months ± 1 year 5 months) included subjects with a mandibular plane angle greater than 28°, y-axis greater than 6°, and SNˆGoGn angle greater than 37°. The low-angle group (30 subjects; 12 male, 18 female; mean age, 19 years 1 month ± 1 year 4 months) consisted of subjects with a mandibular plane angle less than 23°, y-axis less than 63°, and SNˆGoGn angle less than 27°. It was arbitrarily decided that at least 2 of 3 of these variables were required to determine facial type.
The vertical position of the maxillary and mandibular central incisors (L1), mandibular first premolar (L4), and mandibular first (L6) and second (L7) molars were measured perpendicular to the palatal and mandibular planes, respectively. The arch leveling was measured by the changes in the measurements of the distances of those teeth to the mandibular plane.
Dental casts were scanned by a tridimensional scanner (D800; 3Shape A/S, Copenhagen, Denmark) with a scan time of 25 seconds, resolution with 2 cameras at 5.0 megapixels, and ultrahighpoint accuracy less than 15 μm. Each cast was scanned from 10 or more views that were then combined and rendered into 3-dimensional views with the software. The virtual 3-dimensional models were measured and analyzed with the software.
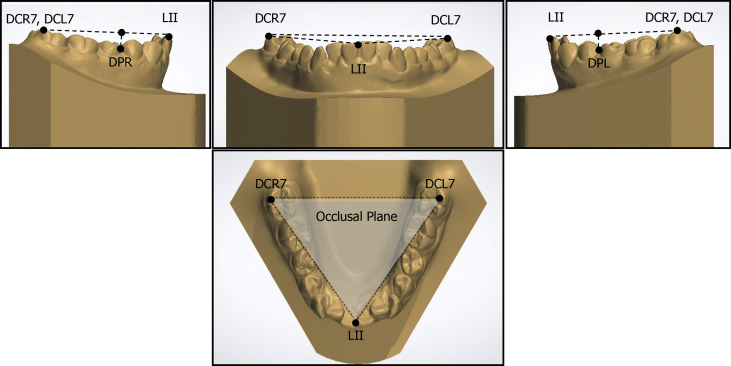
Curve of Spee value was measured as follows: the distobuccal cusps of the left and right second molars and the midpoint between the central incisors served as the 3 landmarks; the occlusal plane, defined by the midpoint of the center in the right and left incisor edges and the tips of the right and left second molar distobuccal cusps, was established in the mandibular dental arch. The perpendicular distances from the occlusal plane to the buccal cusp tip of each lateral tooth were measured. Measurements were obtained on the right and left sides in the deepest points of the curve. Landmarks, reference planes, and measurements used are shown in Figure 3 . The premolar used in measuring the deepest part of the curve of Spee had to be in occlusal contact with an opposing tooth in the maxillary dentition. The curve of Spee value was the summation of the curve of Spee on the right and left sides of the dental arch, and the deepest point was used as a representative value for the curve of Spee on each side.