Because of their multifactorial etiologies, dental and skeletal open bites are among the most difficult malocclusions to treat to a successful and stable result. Etiologic factors include vertical maxillary excess, skeletal pattern, abnormalities in dental eruption, and tongue-thrust problems. The purpose of this article was to report the treatment of an adult patient with a lateral open bite and a unilateral posterior crossbite. The treatment involved nonextraction therapy, including intermaxillary elastics, to obtain dentoalveolar extrusion in the region of the lateral open bite. The treatment results were successful and remained stable 2 years later.
Treatment of an open bite malocclusion can be difficult for the orthodontist, because it develops as a result of the interplay of many etiologic factors. Etiologic factors generally cited in the literature include vertical maxillary excess, skeletal pattern, abnormalities in dental eruption, and tongue-thrust problems. In adults, the mechanical treatment options are limited. Orthognathic surgery is indicated in adult patients with severe open bite and unesthetic facial proportions. For less severe problems, the search for effective treatment modalities continues.
Lateral open bite is rarely observed, especially in adults. In some patients, lateral open bite is due to a disturbance of the eruption mechanism itself, so that nonankylosed teeth cease to erupt. Few lateral open bite cases are reported in the literature, and all involved ankylosed teeth or primary failure of eruption. In this case report, we present the treatment of a patient with a lateral open bite and a unilateral posterior crossbite, treated with fixed appliances and intermaxillary elastics. The treatment results were satisfactory and stable 2 years after the end of active treatment.
Diagnosis and etiology
An 18-year-old man came for orthodontic treatment to the private orthodontic office of the first author (M.C.C.) with a unilateral open bite and a posterior crossbite in centric relation as determined by bilateral manipulation ( Fig 1 ). His chief complaints were an unsatisfactory occlusion, chewing difficulty, and smile esthetics. He reported a tongue-thrusting habit in the open-bite space; this indicated that the lateral open bite was caused by mechanical interference in tooth eruption. There was no previous history of this type of malocclusion in his family, and he had no temporomandibular disorder symptoms.

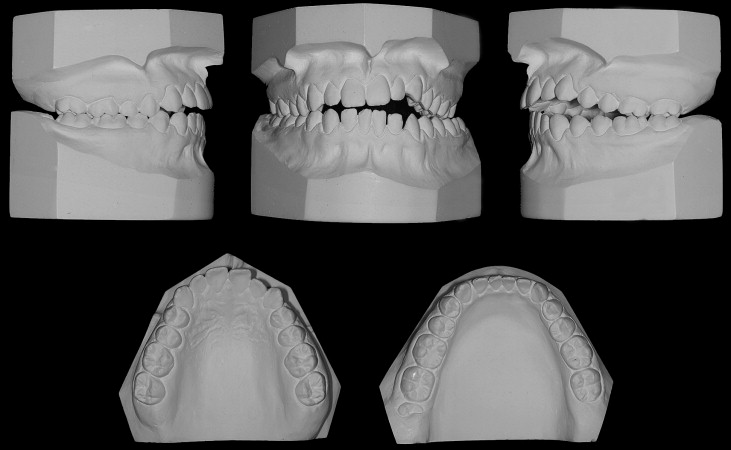
Clinically, the patient had unstrained lip closure, left lateral open bite, and left posterior crossbite ( Fig 1 ). The initial intraoral photographs and dental casts showed a Class I molar relationship on the right side and a Class II molar relationship on the left side, causing a slight maxillary-to-mandibular midline deviation, an overjet of 2 mm, and a left lateral open bite of 3 mm ( Figs 1 and 2 ). The maxillary arch was mildly crowded, and the mandibular arch had mild spacing. The left mandibular third molar was impacted ( Fig 3 ).

The cephalometric analysis showed a convex skeletal profile, an open gonial angle, a narrow and long mandibular symphysis characteristic of the dolicofacial pattern, a deficient maxillomandibular relationship, well-positioned maxillary incisors, and protruded and labially tipped mandibular incisors ( Fig 4 , Table ).

| Pretreatment | Posttreatment | Two years posttreatment | |
|---|---|---|---|
| SNA | 87° | 89° | 89° |
| SNB | 82° | 84° | 85° |
| ANB | 5° | 5° | 4° |
| SND | 81° | 82° | 82° |
| Wits | –1 mm | 1 mm | 2 mm |
| NAP | 8° | 10° | 11° |
| H.NB | 17° | 19° | 17° |
| FMA | 33° | 34° | 32° |
| SN.Occl | 15° | 16° | 15° |
| SN.GoGn | 35° | 36° | 37° |
| N.S.Gn | 68° | 68° | 67° |
| 1.NA | 20° | 19° | 18° |
| 1-NA | 4 mm | 3 mm | 3 mm |
| 1.NB | 32° | 25° | 26° |
| 1-NB | 7 mm | 8 mm | 8 mm |
| IMPA | 94° | 87° | 85° |
| P-NB | 2 mm | 2 mm | 2 mm |
Treatment objectives
The main objectives of the orthodontic treatment were to close the lateral open bite and to correct the left posterior crossbite, to achieve Class I molar and canine relationships on the left side and ideal overjet and overbite. Treatment also aimed to achieve “the 6 keys to normal occlusion” and a mutually protected occlusion, to provide satisfactory facial esthetics and masticatory function, to eliminate the abnormal tongue thrust, and to achieve stable treatment results.
Treatment objectives
The main objectives of the orthodontic treatment were to close the lateral open bite and to correct the left posterior crossbite, to achieve Class I molar and canine relationships on the left side and ideal overjet and overbite. Treatment also aimed to achieve “the 6 keys to normal occlusion” and a mutually protected occlusion, to provide satisfactory facial esthetics and masticatory function, to eliminate the abnormal tongue thrust, and to achieve stable treatment results.
Treatment alternatives
One treatment option was nonextraction therapy, including intermaxillary elastics to correct the left posterior crossbite and to obtain dentoalveolar extrusion in the region of the lateral open bite.
Another treatment option consisted of surgically assisted rapid maxillary expansion to correct the left posterior crossbite and subsequent use of intermaxillary elastics to close the lateral open bite. Rapid maxillary expansion without surgical assistance was also a treatment option, in spite of the patient’s age, to achieve at least buccal inclination of the maxillary posterior teeth.
The patient rejected the surgically assisted rapid maxillary expansion and preferred the first treatment alternative.
Treatment planning
Because the patient had an acceptable profile and minimal arch-length discrepancy, nonextraction treatment was planned. The left posterior crossbite would be corrected with intermaxillary elastics. The lateral open bite would be closed by extruding the maxillary left lateral incisor, canine, and premolars. Because this procedure is reportedly prone to relapse, he would need myofunctional therapy after the orthodontic treatment.
Treatment progress
All third molars were extracted before fixed appliance placement. Treatment was started simultaneously in the mandibular and maxillary arches, with a straight-wire appliance (0.022 × 0.028 in, A Company, San Diego, Calif). Initially, nickel-titanium archwires were used (0.016 and 0.018 in). After 4 months of treatment, when the teeth were relatively level and aligned, stainless steel archwires were used (0.014, 0.016, and 0.018 in), and the maxillary archwire was slightly expanded in the posterior region. At this time, intermaxillary elastics were used from the palatal buttons on the bands of the left maxillary molars to the buccal hooks on the mandibular left molars. These intermaxillary elastics helped to correct the posterior crossbite ( Fig 5 ). Subsequently, vertical intermaxillary elastics were used in 2 dental segments: 1 linking the maxillary and mandibular left lateral incisor and canines, and the other linking the maxillary and mandibular left premolars and first molars ( Fig 5 ). The patient was instructed to change the elastics daily. Intermaxillary elastics were used for 5 months until a normal vertical bite relationship was achieved. Because the maxillary incisal and posterior occlusal planes were oblique and not parallel to the interpupillary line, and the mandibular incisal and posterior occlusal planes were slightly canted in the opposite direction, rectangular archwires were used in the mandibular arch and round archwires in the maxillary arch, with vertical elastics, to allow bite closing with greater extrusion of the maxillary teeth and less extrusion of the mandibular teeth, while correcting the asymmetric canting of both dental arches ( Fig 5 ). After open-bite closure, the vertical elastics were maintained for an additional 5 months. Thereafter, the elastics were removed, and leveling archwires were placed for 5 months to determine the open-bite relapse potential. The Class II molar relationship on the left side was corrected with Class II elastics during the alignment phase. After the fixed appliances were removed, a modified Hawley retainer was placed in the maxillary arch, a canine-to-canine mandibular retainer was bonded, and the patient received myofunctional therapy. Active treatment time was 2 years 9 months.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


