This case report describes the interdisciplinary treatment of a 39-year-old man with several missing teeth (including both maxillary lateral incisors), Class II malocclusion, deep overbite, and significant mandibular midline deviation. The treatment plan included placement of endosseous dental implants early in the orthodontic treatment to increase the vertical dimension of the occlusion for deepbite correction, canine substitution for the missing lateral incisors, and distalization of the mandibular right buccal segment with the aid of a temporary anchorage device.
Effective and efficient orthodontic management of partially edentulous patients is biomechanically challenging and often requires a thorough treatment plan to predictably achieve the desired tooth movements. Comprehensive orthodontic treatment in adults with several missing teeth requires an interdisciplinary approach to restore the occlusion. Associated with the missing teeth, these patients often have edentulous ridges with reduced buccolingual and vertical dimensions, altered occlusal planes caused by extrusion of unopposed teeth, migration of teeth into adjacent extraction spaces, and associated periodontal defects.
In patients with several missing teeth, certain types of tooth movement are significantly challenging with conventional mechanics. Overbite reduction, distalization, intrusion of posterior teeth, and retraction of anterior teeth are some movements that require a full complement of teeth in the buccal segments to minimize the side effects. Proffit et al advocated skeletal anchorage devices for intrusion of posterior teeth, distalization of molars or the entire arch, retraction and intrusion of protruding maxillary incisors, and positioning of individual teeth when no other satisfactory anchorage is available. When restorative implants are used as an alternative or adjunctive to miniscrews, most of these types of tooth movements are possible in these patients. Endosseous dental implants can be used for anchorage in these patients and also to increase or support the increased vertical dimension of the occlusion in adults with deep overbite and to reestablish the esthetics of the smile in the early phases of orthodontic treatment.
This case report describes the interdisciplinary team approach for a partially edentulous patient with endosseous dental implants placed early in the orthodontic treatment to increase the vertical dimension, a temporary anchorage device for unilateral en-masse distalization in the mandibular arch to correct a significant midline deviation and anterior crowding, and canine substitution for the congenitally missing lateral incisors.
Etiology and diagnosis
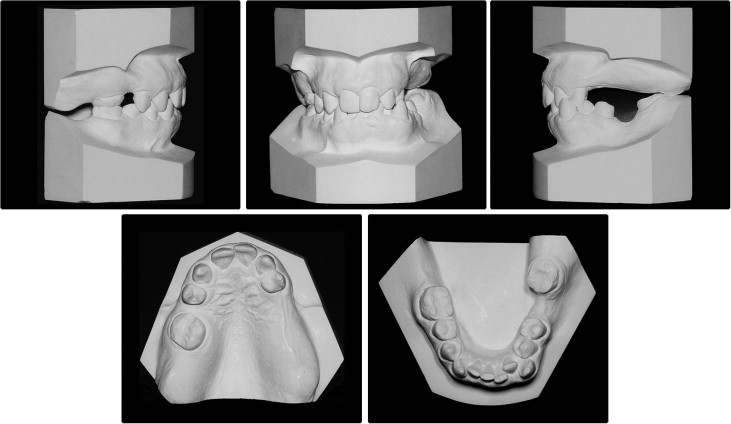
A man, aged 39 years, with multiple missing teeth was referred by his prosthodontist for interdisciplinary treatment. His chief complaint was the missing teeth, and he wanted an esthetic smile. His medical history was noncontributory, and the extraoral examination showed facial symmetry, a convex soft-tissue profile caused by a retrognathic mandible, competent lips at rest, and an obtuse nasolabial angle ( Fig 1 ). He had a flat smile arc with asymmetric animation of the smile. There were no signs of temporomandibular joint disorders.

Intraorally, the patient had congenitally missing maxillary lateral incisors and third molars. Additionally, the maxillary right second molar and first premolar; maxillary left second premolar and first and second molars; mandibular left first molar; and mandibular right second molar were lost due to dental caries ( Fig 2 ). As a result, supereruption and migration of teeth into the adjacent extraction spaces was observed. The maxillary dental midline was shifted to the right by 1 mm, and the mandibular dental midline was shifted by 4 mm to the left relative to the facial midline. The canines on the left side were in crossbite. Overbite was 5 mm, and overjet was normal. The molar relationship was Class II on the right side. The canine relationships were Class I on the right and Class II on the left. There was 4 mm of anterior spacing in the maxillary arch and 3 mm of residual edentulous space mesial to the maxillary right first molar. Arch length-tooth size discrepancy of 6 mm was evident in the mandibular arch, not considering the edentulous 9-mm space of the missing mandibular left first molar. The second molar was mesially tipped and supererupted.
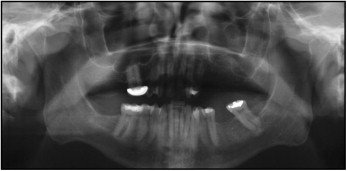
The panoramic radiograph ( Fig 3 ) showed large restorations on the mandibular right first molar, mandibular left second molar, and maxillary left first premolar, and a full-coverage restoration on the maxillary right first molar. The cephalometric analysis ( Fig 4 ; Table ) indicated a mild Class II skeletal base, and a convex soft- and hard-tissue profile caused by the retrognathic mandible in relation to the cranial base. Vertically, the patient had a slightly increased mandibular plane angle. The maxillary and mandibular incisors were retroclined, and the upper and lower lips were retrusive in relation to the E-line. Periodontal health was adequate, with no probing depth greater than 4 mm.

| Variable | Norm | Pretreatment | Posttreatment | Change |
|---|---|---|---|---|
| SNA (°) | 82 | 81.2 | 81.8 | 0.6 |
| SNB (°) | 80 | 78.7 | 77.7 | 1 |
| ANB (°) | 2 | 2.5 | 4.1 | 1.6 |
| FMA (°) | 25 | 30.6 | 33.3 | 2.7 |
| IMPA (°) | 90 | 85.2 | 85 | 0.2 |
| U1-NA (°) | 22 | 19.8 | 19 | 0.8 |
| U1-NA (mm) | 4 | 4.1 | 3 | 1.1 |
| L1-NB (°) | 25 | 19.8 | 21.4 | 1.6 |
| L1-NB (mm) | 4 | 4.1 | 5 | 0.9 |
| Interincisal angle (°) | 131 | 136.9 | 138.1 | 1.2 |
| Upper lip to E-line (mm) | −6 | −3.8 | −4.2 | −0.4 |
| Lower lip to E-line (mm) | −2 | −1.2 | −2 | −0.8 |
Treatment objectives
The treatment objectives were to (1) maintain the facial profile, (2) achieve normal overbite and overjet, (3) restore prosthetically the missing teeth, (3) alleviate crowding in the mandibular anterior region, (4) correct the mandibular dental midline, and (5) improve smile esthetics.
Treatment objectives
The treatment objectives were to (1) maintain the facial profile, (2) achieve normal overbite and overjet, (3) restore prosthetically the missing teeth, (3) alleviate crowding in the mandibular anterior region, (4) correct the mandibular dental midline, and (5) improve smile esthetics.
Treatment alternatives
Opening space for the missing lateral incisors for implant-supported crowns is a possible approach for the management of missing maxillary lateral incisors instead of canine substitution. However, with this approach, the number of necessary skeletal anchorage units in the maxilla would have to increase, one in each quadrant, to retract the canines with maximum anchorage. Furthermore, the similar morphology of the maxillary premolars to that of a canine also influenced the treatment plan in favor of canine substitution.
Extraction of a mandibular incisor could have been considered. However, this approach would still require 2 mm of distalization of the mandibular right buccal segment to achieve an adequate occlusion.
Finally, mandibular left second molar intrusion and protraction into the first molar extraction space was an option. Intrusion of the molar by 4 mm and protraction of 6 mm into the long-standing edentulous space would be difficult and time-consuming; thus, extraction of the second molar with a prosthodontic implant for the missing first molar was considered.
All treatment options were discussed, and the patient decided to have canine substitution and endosseous dental implants for the missing teeth.
Treatment plan
- 1.
Bilateral canine substitution for the missing maxillary lateral incisors with subsequent reshaping and composite restorations of the substituted canines.
- 2.
Placement of provisional crowns on the maxillary right first molar to increase the vertical dimension of the occlusion by 2 to 3 mm anteriorly.
- 3.
Placement of endosseous dental implants in the sites of the maxillary left first molar and second premolar with temporary crowns fabricated to support the newly established vertical dimension of the occlusion.
- 4.
Distalization of the mandibular right segment by 3 mm to alleviate the crowding and shift the midline to the right side using a skeletal anchorage device.
- 5.
Elimination of the left canine crossbite and achieve normal overbite.
- 6.
Open space for a maxillary right second premolar endosseous dental implant by distalization of the first molar to maintain the Class II molar relationship and a 3-mm protraction of the first premolar and canine while shifting the midline to the left by 1 mm.
- 7.
Extraction of the mandibular left second molar and placement an endosseous dental implant for the missing first molar after the orthodontic treatment.
- 8.
Maintenance of the facial profile.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


