Introduction
Virtual 3-dimensional (3D) models obtained by scanning of physical casts have become an alternative to conventional dental cast analysis in orthodontic treatment. If the precision (reproducibility) of virtual 3D model analysis can be further improved, digital orthodontics could be even more widely accepted. The purpose of this study was to clarify the influence of “standardization” of the target points for dental cast analysis using virtual 3D models. Physical plaster models were also measured to obtain additional information.
Methods
Five sets of dental casts were used. The dental casts were scanned with R700 (3Shape, Copenhagen, Denmark) and REXCAN DS2 3D (Solutionix, Seoul, Korea) scanners. In this study, 3 system and software packages were used: SureSmile (OraMetrix, Richardson, Tex), Rapidform (Inus, Seoul, Korea), and I-DEAS (SDRC, Milford, Conn).
Results
Without standardization, the maximum differences were observed between the SureSmile software and the Rapidform software (0.39 mm ± 0.07). With standardization, the maximum differences were observed between the SureSmile software and measurements with a digital caliper (0.099 mm ± 0.01), and this difference was significantly greater ( P <0.05) than the 2 other mean difference values. Furthermore, the results of this study showed that the mean differences “WITH” standardization were significantly lower than those ”WITHOUT“ standardization for all systems, software packages, or methods.
Conclusions
The results showed that elimination of the influence of usability or habituation is important for improving the reproducibility of dental cast analysis.
Highlights
- •
The reproducibility of dental cast analysis with virtual 3-dimensional models was clarified.
- •
Elimination of the influence of usability or habituation is important.
- •
Standardization was highly effective for improving the reproducibility.
- •
Dental cast analysis with physical casts is still difficult with a digital caliper.
Virtual 3-dimensional (3D) models obtained by scanning of physical casts have become an alternative to conventional dental cast analysis in orthodontic treatment. In general, physical models have problems in clinical practice because they can be lost, fractured, or degraded, and they require physical storage space. In contrast, virtual 3D models are easy to store and transport with electronic data transfer. Earlier studies have shown that measurements of tooth width and dental arch width with a caliper and plaster casts show equal or less variability than measurements based on software programs with virtual 3D digital models. Commercially available virtual 3D models can be produced by direct or indirect methods. Indirect methods begin with dental impressions. Virtual 3D models can then be obtained by laser scanning of the physical models or computed tomography imaging of the impressions or physical models. The direct method uses an intraoral scanner to directly scan the patient’s dentition. Recently, the validity of virtual 3D models produced with an indirect method was evaluated in a systematic review by assessing the agreement between measurements of the virtual and physical models. The conventional technique showed better overall reproducibility and thus appears to be more suitable for scientific work. However, the reproducibility obtained with a virtual 3D model was still clearly acceptable for clinical use. A recent article showed that linear measurements taken on virtual 3D models are accurate and reproducible. Virtual 3D models obtained with a surface laser scanner are reliable for measurements of arch width and length. No statistically significant differences were found between the physical and digital measurements of arch width and length in dental models. However, the maximum value of the mean difference between these methods was 0.888 mm. Another recent study also showed that the accuracy of the software used for the spatial analysis of virtual 3D models is clinically acceptable, and the results are comparable to those achieved with traditional plaster models. Furthermore, the mean difference between the virtual and physical models was 0.456 mm. A recent concern about 3D virtual models is that most studies have not indicated that the use of virtual 3D models would cause an orthodontist to make a different diagnosis of the malocclusion than he or she would make using physical models; ie, virtual 3D models are not a suitable choice for treatment planning or diagnosis. Im et al concluded that digital models require the delicate adjustment of proximal and occlusal contacts because of the possibility of collision. If the precision (reproducibility) of virtual 3D model analysis can be further improved, digital orthodontics may become more widely accepted.
The purpose of this study was to clarify the influence of “standardization” of the target points for dental cast analysis by using virtual 3D models. Furthermore, the effectiveness of such standardization for the measurement of physical plaster models was also assessed for additional information. In this study, 3 system or software packages and the caliper method were used to assess the influence of standardization to eliminate the usability or habituation.
Material and methods
In this study, 5 sets of dental casts were used. All 5 sets were scanned with an R700 3D scanner (3Shape, Copenhagen, Denmark). The manufacturer claims that the R700 is accurate to ±0.02 mm. A REXCAN DS2 3D scanner (Solutionix, Seoul, Korea) was also used in this study. The manufacturer claims that the REXCAN DS2 is accurate to ±0.02 mm. In this study, 3 system or software packages were used: SureSmile (OraMetrix, Richardson, Tex), Rapidform (Inus, Seoul, Korea), and I-DEAS (SDRC, Milford, Conn). With SureSmile, the scanned data were sent via the Internet through a firewall connection to the digital laboratory at OraMetrix, where technicians created digital models (shell model, gingiva model, model base, teeth model, and so on). The shell model is created by denoising and refining the registration of raw scanned data, and this model is then used to create the other models. For Rapidform and I-DEAS, denoising and refinement of the registrations were carried out by a research assistant (O.C.).
For the shell-shell deviations of the 3D virtual models, the models were based on different 3D scanning data obtained by the R700 and REXCAN DS2 and were also created by different processes. The accuracy of each 3D virtual model was assessed by calculation of the shell-shell deviations. An OrthoCAD model (Align Technology, San Jose, Calif) based on R700 data has been reported to be highly accurate. Thus, an OrthoCAD model that was obtained previously was used as a standard model. The shell-shell deviations in each comparison were determined by applying the least-squares method to register each model (all 5 sets) using 3D reverse-engineering software (Rapidform; Inus). In this study, the maximum mean deviation set as a registration threshold was 0.01 mm, and was expressed as
where Xi is each value in the data set, X is the mean of all values in the data set, and n is the number of values in the data set. In this study, the root mean square error (also called the root mean square deviation) was calculated for each registration between the 3D models.
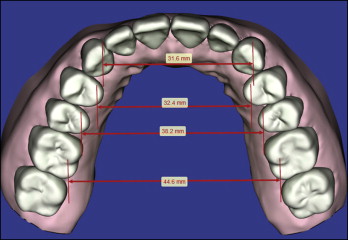
For dental cast analysis “WITHOUT” standardization of the target points, the measured parameters regarding arch widths were compared among the system or software methods. In the SureSmile system (SureSmile treatment software), 3D distances between canines, premolars, and molars were calculated by a digital laboratory ( Fig 1 ). The measured values obtained with the SureSmile software were used as references (gold standards) for comparison in this study because the SureSmile models are the most accurate, as assessed in terms of the mean square error. Next, the 3 different methods (2 software packages, and a caliper method) were compared with the values obtained with the SureSmile software: Rapidform and I-DEAS software were used to measure each arch width. All measurements in all 10 virtual 3D models were performed 3 times for each parameter by the same research assistant (O.C.) without standardization of the target points. Before the measurements, the research assistant was instructed to measure between the tips of the canines, the lingual cusp tips of the premolars, and the distolingual cusp tips of the first molars, as shown in Figure 1 . Both software applications can calculate 3D distances between 2 arbitrary points ( Fig 2 ). A digital caliper was also used. For all parameters, 3 measurements were made by the same research assistant. The values were averaged over the 10 3D dental casts. The means of the total differences of the measured values between the SureSmile system and the 3 different methods (2 software packages, and a caliper method) were calculated and compared.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


