This case report describes the orthodontic treatment of an adult patient with iatrogenic absence of the maxillary canines, moderate maxillary and severe mandibular dental crowding, a Bolton discrepancy with a large mandibular anterior excess, a maxillary right lateral incisor crossbite, and Angle Class II molar relationships. The treatment consisted of fixed appliance therapy, mandibular incisor extraction, tooth bleaching, and dental recontouring. This method of treatment maintained the patient’s good facial appearance, improved the dental esthetics, and provided a good functional occlusion, eliminating the arch length and Bolton discrepancies and providing a good outcome with minimal undesirable effects.
The orthodontic treatment of a malocclusion with no canines is not a common condition. Permanent canine agenesis is rare, and maxillary canines can be positioned variably. They can be palatably or labially displaced, and the possibility of prior extraction should be assessed by the clinician. Canine extraction as a treatment goal is rare; thus, this condition can be called iatrogenic absence of the canines, which has not been well explored in the literature. In contrast, the situation of ectopically erupted canines might require extraction because of the difficult position and complicated orthodontic traction. Many investigators claim that a tooth-size discrepancy is an important element in diagnosis and should be measured in each orthodontic patient before starting treatment. However, when there are no maxillary canines, the Bolton discrepancy is evident; when associated with dental crowding and an Angle Class II molar relationship, it creates a more complicated treatment. It remains questionable whether a Bolton discrepancy from the absence of canines always affects the final orthodontic treatment outcome.
Agenesis of canines, maxillary central incisors, and first premolars is relatively rare when all third molars are present. However, iatrogenic absence of the maxillary canines associated with mandibular incisor extraction treatment is an uncommon condition that is not described in the literature. Therefore, the purpose of this case report was to describe the treatment of an adult patient with iatrogenic absence of the maxillary canines, moderate maxillary and severe mandibular crowding, a Bolton discrepancy with a large mandibular anterior excess, a maxillary right lateral incisor crossbite, and Angle Class II molar relationships.
Diagnosis and etiology
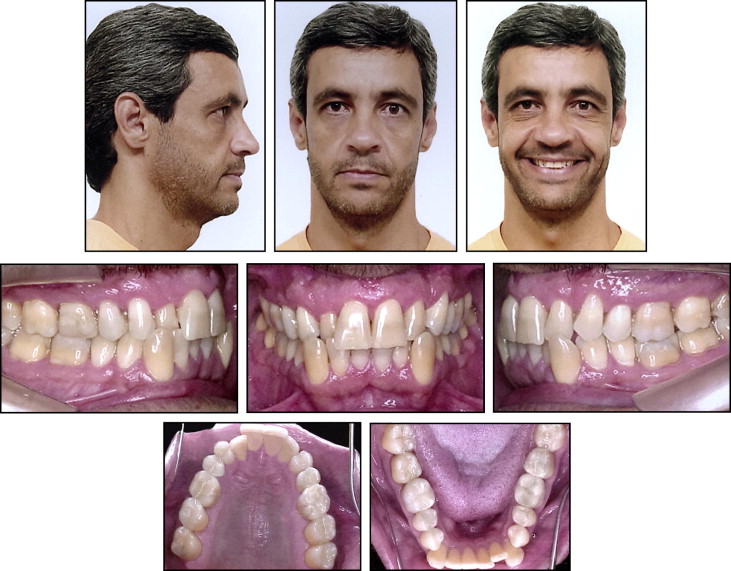
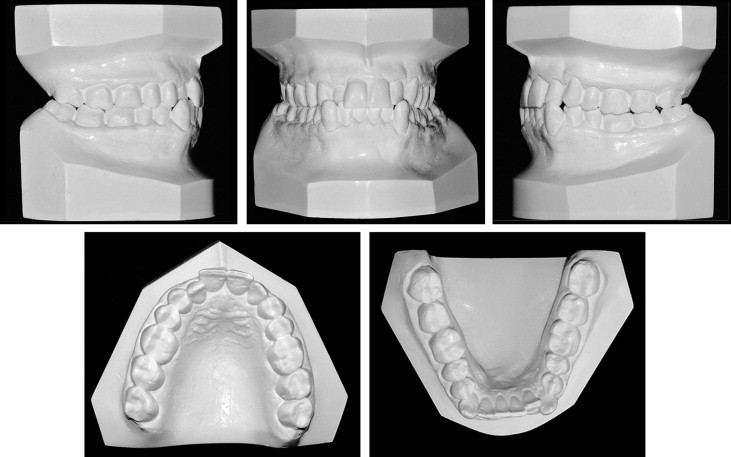
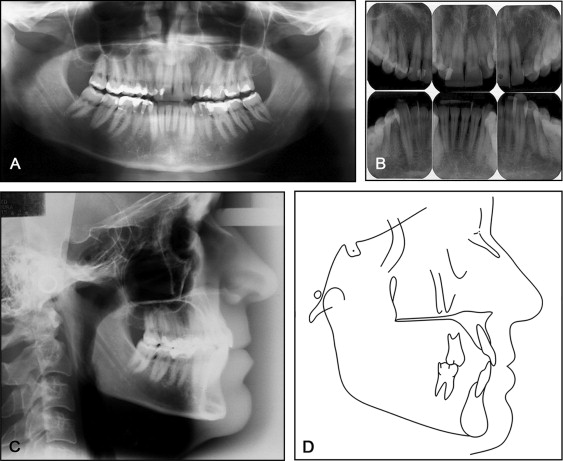
A 47-year-old man was referred for orthodontic treatment with the chief complaint of maxillary and mandibular dental crowding. The intraoral examination showed iatrogenic absence of the maxillary canines, a maxillary right lateral incisor crossbite, worn incisal edges, and Angle Class II molar relationships. The arch-length discrepancies were −2.8 mm in the maxillary arch and −6.3 mm in the mandibular arch ( Figs 1 and 2 ). The Bolton overall ratio was 110.12, and the anterior ratio was 119.04. The tooth-size discrepancy showed a 6.6-mm mandibular anterior excess. Therefore, the patient’s maxillary arch was too small for his mandibular arch because of the iatrogenic absence of the maxillary canines. Also, he had gingival recession of the mandibular left canine and worn incisor edges. The maxillary midline was coincident with the facial midline and the mandibular midline. His dental history indicated that the erupted maxillary canines had been extracted by a dentist because of severe crowding in the maxillary arch. There was no history of oral habits, and his medical history indicated no serious illnesses. The Angle Class II molar relationship was probably due to the iatrogenic absence of the maxillary canines. Thus, the maxillary posterior segment was displaced mesially, and it was determined to be a right Class II complete malocclusion and a left Class II three quarters molar malocclusion ( Figs 1 and 2 ). The panoramic and periapical radiographs showed good periodontal health ( Fig 3 ). The profile was straight, with good facial balance and lip competence. The cephalometric analysis showed that all skeletal and dental relationships were within normal limits ( Table ).
| Measurement | Standard values | Pretreatment | Posttreatment |
|---|---|---|---|
| SNA ( o ) | 82 | 86 | 85 |
| SNB ( o ) | 80 | 84 | 83 |
| ANB ( o ) | 2-4 | 2 | 2 |
| FMA ( o ) | 25 ± 3 | 22.5 | 23 |
| SN.GoGn ( o ) | 32 ± 3 | 28 | 29.5 |
| Mx1.PP ( o ) | 110 ± 5 | 109 | 110 |
| IMPA ( o ) | 90 ± 5 | 90 | 89 |
| Overjet (mm) | 3 | 3 | 3 |
| Overbite (mm) | 3 | 3 | 2 |
| Upper lip to S-line (mm) | 0 | −3.5 | −3.5 |
| Lower lip to S-line (mm) | 0 | −1.5 | −1.5 |
Treatment objectives
The treatment objectives were to (1) eliminate the maxillary and mandibular arch-length discrepancies, (2) correct the maxillary right lateral incisor crossbite, (3) eliminate the Bolton discrepancy with compensation for the relative excess mandibular tooth size with mandibular incisor extraction, (4) substitute the maxillary first premolars for the canines and the second premolars for the first premolars, (5) maintain the Class II molar relationships and facial balance, and (6) restore the incisal edges plus tooth bleaching to improve the dental esthetics.
Treatment objectives
The treatment objectives were to (1) eliminate the maxillary and mandibular arch-length discrepancies, (2) correct the maxillary right lateral incisor crossbite, (3) eliminate the Bolton discrepancy with compensation for the relative excess mandibular tooth size with mandibular incisor extraction, (4) substitute the maxillary first premolars for the canines and the second premolars for the first premolars, (5) maintain the Class II molar relationships and facial balance, and (6) restore the incisal edges plus tooth bleaching to improve the dental esthetics.
Treatment alternatives
Based on the objectives, 2 treatment options were presented to the patient. One option was to extract 2 mandibular premolars, and the other option consisted of extracting the mandibular left central incisor. A diagnostic wax-up was required to predetermine the occlusal possibilities; it showed that both treatment protocols would eliminate the arch-length and Bolton discrepancies. However, the wax-up showed that the 2 mandibular premolar extractions would not improve the occlusion as well as the mandibular incisor extraction. Thus, the mandibular incisor extraction approach was the best treatment option. The main advantage of this treatment would be to eliminate the chief complaint, which was the maxillary and mandibular dental crowding. The Bolton discrepancy caused by the iatrogenic absence of the maxillary canines would be eliminated by extracting the mandibular left central incisor and substituting the maxillary first premolars as the canines and the second premolars as the first premolars. The maxillary and mandibular arch-length discrepancies would be eliminated by maxillary anterior tooth stripping and mandibular left central incisor extraction.
Treatment progress
M.B.T. (Morelli, Sorocaba, São Paolo, Brazil) prescription 0.022 × 0.028-in slot fixed appliances were used; because the canines were absent, canine brackets were placed on the first premolars. Glass ionomer cement was placed on the molar occlusal surfaces to increase the vertical dimension to correct the maxillary right lateral incisor crossbite. A continuous 0.016-in nickel-titanium archwire was placed with an open-coil spring to obtain space between the maxillary right first premolar and the central incisor. After extraction of the mandibular left central incisor, leveling and alignment were accomplished with the usual wire sequence of 0.014-in nickel-titanium, followed by 0.016-, 0.018-, and 0.020-in round stainless steel archwires. Rectangular archwires were inserted to control the torque of the anterior teeth, detail the occlusion, and parallel the roots in the extraction site. Class III elastics were used to improve the canine relationships. After correcting the maxillary right lateral incisor crossbite, the glass ionomer cement was removed. The maxillary midline coincided with the center of the remaining mandibular central incisor. After the treatment, the patient was referred to a general dentist to recontour the maxillary first premolars as canines and to restore the maxillary and mandibular incisors edges, thus improving dental esthetics. The patient was retained with a maxillary bonded lateral incisor-to-lateral incisor retainer and a mandibular bonded canine-to-canine retainer with 0.020-in braided archwires. Total active treatment time was 1 year 5 months.
Treatment results
The facial photographs show that the patient has a harmonious relationship of the soft tissues and a pleasant facial profile, with passive lip competence. The maxillary dental midline was coincident with the facial midline and with the center of the remaining mandibular central incisor ( Figs 4 and 5 ). The intraoral photographs show that the arch-length discrepancies were eliminated, and the maxillary right lateral incisor crossbite was corrected. The Bolton discrepancy created by the iatrogenic maxillary canines was eliminated with the mandibular left central incisor extraction and with the Class I bilateral canine occlusion modified by the presence of the maxillary first premolars. Thus, normal anterior overjet and overbite relationships were obtained ( Table , Figs 4-6 ). The panoramic radiograph shows good root parallelism, normal bone levels, and little root resorption. There was improvement in the gingival recession in the mandibular left canine area ( Fig 6 ). Cephalometric superimposition on the sella-nasion plane and on the palatal curve showed no difference in the maxillary and mandibular incisor inclinations, which helped to maintain lip competence, despite the mandibular left central incisor extraction ( Table , Fig 7 ).



