Introduction
There is a lack of research to support the belief that root canal treatment can be considered for stopping or decreasing external apical root resorption (EARR). There is conflicting evidence as to whether root-filled teeth are more or less likely to experience EARR after orthodontic treatment. The purpose of this study was to compare the degree of EARR of root-filled teeth with that of contralateral teeth with vital pulp after fixed orthodontic treatment.
Methods
The study sample consisted of 35 patients aged 25.23 ± 4.92 years who had at least 1 root-filled tooth before orthodontic treatment. Digital panoramic radiographs of each patient taken before and after orthodontic treatment were used to measure the EARR. The Student t test for matched pairs and the Pearson correlation analysis were applied.
Results
The mean EARR values were 0.22 (0.14, 0.35) for root-filled teeth and 0.87 (0.59, 1.31) for contralateral teeth with vital pulp, indicating significantly less EARR for root-filled teeth compared with the contralateral teeth with vital pulp after orthodontic treatment. EARR was influenced by the patient’s age, treatment duration, treatment type, and periapical pathosis, but not by tooth type and sex.
Conclusions
Root-filled teeth appear to be associated with significantly less EARR than are contralateral teeth with vital pulp. This study suggests that the possible complication of EARR in root-filled teeth may not be an important consideration in orthodontic treatment planning, and root canal treatment can be considered for stopping or decreasing EARR when severe EARR occurs during orthodontic treatment.
Highlights
- •
Root-filled and contralateral teeth with vital pulp were compared after orthodontics.
- •
Root-filled teeth had less external apical root resorption (EARR) than the contralaterals.
- •
EARR of root-filled teeth might not be significant in orthodontic treatment planning.
External apical root resorption (EARR) is a type of surface resorption and an undesirable result of orthodontic treatment that can lead to loss of tooth structure. External root resorption occurs from all directions, including both the apical region and the sides of the root, whereas EARR of teeth undergoing orthodontic treatment shows only apical resorption with no ankylosis and an intact periodontal ligament, and the resorbed apical root portion is replaced with normal bone when treatment is discontinued.
Massler and Malone observed EARR in 86.4% of orthodontic patients. Histologic studies have reported that EARR occurs in more than 90% of orthodontic patients. The life and normal function of a tooth is unaffected in most cases of mild EARR, but in some cases of severe EARR, orthodontic treatment should be halted.
Many factors can initiate and induce EARR during orthodontic treatment, including age, sex, nutrition, genetics, type of orthodontic appliance, force magnitude, tooth extraction, treatment duration, and distance of tooth movement.
It is suggested that contact between the root and the alveolar bone could cause EARR, but a relationship between EARR and pulp has also been reported. Pulp tissue can be damaged by trauma from orthodontic tooth movement. Since pulp vessels are branches of alveolar bone vessels, heavy orthodontic forces can damage apical vessels, and a tipping force can stretch the apical vessel and result in pulpal disturbance. It was also reported that pulpal disturbances are caused by decreased blood flow after continuous light orthodontic tipping forces are applied.
There seems to be little difference in the movements of root-filled teeth (RFT) and contralateral teeth with vital pulp (VPT). However, there is conflicting evidence as to whether RFT are more or less likely to experience EARR after orthodontic treatment.
We compared the amounts of EARR between RFT and VPT after fixed orthodontic treatment in 35 patients, and evaluated the relationship between EARR and contributing factors such as sex, age, tooth type, periapical pathosis, orthodontic treatment duration, and treatment type (whether teeth were extracted).
Material and methods
Measurements of EARR in RFT and contralateral VPT were taken before and after orthodontic treatment using digital panoramic radiographs, and the relationship between EARR and contributing factors such as sex, age, tooth type, periapical pathosis, orthodontic treatment duration, and treatment type (whether teeth were extracted) was evaluated. The study was approved by the institutional review board for human studies of Yeouido St Mary’s Hospital, College of Medicine, Catholic University of Korea in Seoul (number SC14RISI0100).
This study included 35 patients (8 men, 27 women) aged 25.23 ± 4.92 years, who were selected from patients treated in the orthodontic department our institution from 2006 to 2014. The duration of orthodontic treatment exceeded 1 year (26.58 ± 8.58 months). Inclusion criteria were as follows: (1) RFT before orthodontic treatment, (2) contralateral VPT with radiographically normal periapical anatomic structures (intact periodontal ligament space and lamina dura) diagnosed by clinical examinations, (3) orthodontic treatment exceeding 1 year, and (4) only teeth with no changes on the incisal or occlusal edge confirmed by a cast before and after orthodontic treatment. All 35 patients were treated with conventional brackets (Roth prescription, slot 0.022-in). Treatments of all patients were performed with a general archwire sequences of a 0.016-in nickel-titanium to 0.019 × 0.025-in stainless steel (G&H Orthodontics, Franklin, Ind).
For each patient, a chart review was performed to obtain the clinical examination results. The inclusion criteria for the VPT were the following: (1) no clinical signs or symptoms (no history of pain, swelling, fistula, crown discoloration, percussion sensitivity, or tooth mobility), (2) no untreated dental caries (radiographically confirmed), and (3) no history of other dental treatment during orthodontic treatment.
We used digital panoramic radiographs taken at the first dental examination before orthodontic treatment and at orthodontic debonding. Two trained radiology assistants using the same digital orthopantomograph machine (Promax standard type, 80 kV; Planmeca, Helsinki, Finland) took the radiographs at both times for each patient. A positioning light was used to standardize the head position. The images were obtained using the m-view program (Marosis; INFINITT Healthcare, Seoul, Korea). In all cases, the radiographs showed the entire coronoapical length of the measured teeth, with a clearly defined apex. The images were displayed on a monitor (L1910; Hewlett-Packard, Palo Alto, Calif) using an HD graphic card (Intel, Santa Clara, Calif) with 32-bit quality color and 1280 × 1024 pixels of resolution.
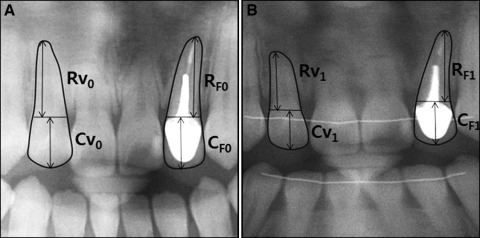
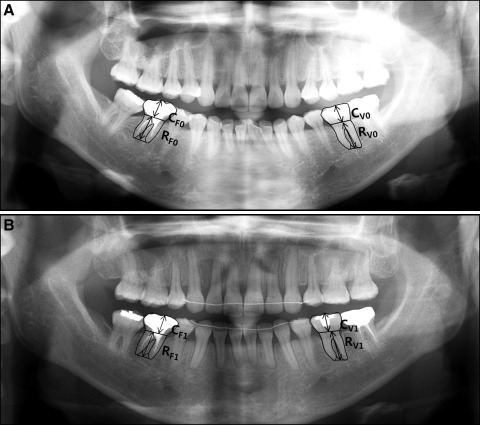
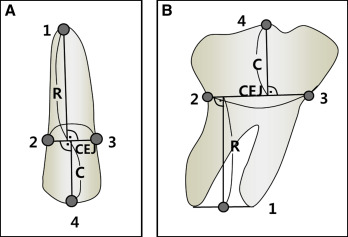
The lengths of crowns and roots were measured using the m-view program. The reference points and lines for measurements before and after orthodontic treatment are shown in Figures 1 and 2 . Crown and root lengths were measured using the method of Linge and Linge ( Fig 3 ). First, the cementoenamel junction (CEJ) was determined as a straight line between 2 points, the mesial and distal CEJs. Next, crown lengths in the initial and final radiographs were calculated in the RFT and VPT by measuring the greatest distance from the incisal or occlusal edge to the CEJ. Root lengths in the initial and final radiographs were also calculated in the RFT and VPT by measuring the distance from the CEJ to the root apices. The root lengths of teeth with multiple roots were calculated by measuring the distance from the CEJ to the middle point on the line between the root apices.
EARR for RFT was calculated as follows: root length before orthodontic treatment − root length after orthodontic treatment × (crown length before orthodontic treatment/crown length after orthodontic treatment).
The amount of EARR was calculated in millimeters. The proportion of EARR for each RFT/VPT pair was calculated as follows: proportion of EARR = EARR in RFT/EARR in VPT.
The difference in EARR for each pair was calculated as follows: difference in EARR = EARR in RFT–EARR in VPT.
Statistical analysis
The Student t test for matched pairs and the Pearson correlation analysis were applied. The level of statistical significance was set at P < 0.05. The same clinician (Y.J.L.) performed all assessments of root resorption. Ten patients were randomly selected, and 20 panoramic radiographs before and after orthodontic treatment were measured by the same examiner after a 10-day interval to determine reliability ( Table I ). The intraclass correlation coefficient between the 2 examinations was 0.98 (0.93-0.99). The difference between the first and second measurements was not significant.
| Patient | First measurement | Second measurement | ||
|---|---|---|---|---|
| EARR for RFT | EARR for VPT | EARR for RFT | EARR for VPT | |
| 1 | 0.96 | 1.49 | 1.03 | 1.30 |
| 2 | 1.09 | 3.29 | 1.10 | 3.34 |
| 3 | 0.71 | 0.97 | 0.81 | 1.07 |
| 4 | 0.10 | 0.90 | 0.10 | 0.93 |
| 5 | 0.10 | 2.52 | 0.26 | 2.65 |
| 6 | 0.06 | 0.60 | 0.09 | 0.71 |
| 7 | 0.05 | 0.10 | 0.08 | 0.13 |
| 8 | 0.35 | 3.04 | 0.32 | 3.10 |
| 9 | 0.11 | 4.53 | 0.07 | 4.67 |
| 10 | 0.07 | 0.11 | 0.10 | 0.14 |
Results
Table II shows the amount of EARR in each type of tooth for each patient. Overall, 31 of the 35 subjects (88.57%) had more EARR in RFT than in VPT. Four patients (11.43%) had the opposite ( P < 0.0001).
| Patient | Sex | Age (y) | Treatment duration (mo) | Treatment type | Tooth type | Periapical lesion (before) | Periapical lesion (after) | EARR in RFT | EARR in VPT | Difference in EARR | Proportion of EARR |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 17 | 35 | 1 | CI | 0 | 0 | 0.06 | 2.14 | −2.08 | 0.03 |
| 2 | F | 26 | 28 | 1 | CI | 0 | 0 | 0.71 | 0.97 | −0.27 | 0.73 |
| 3 | F | 32 | 27 | 0 | CI | 1 | 1 | 1.29 | 1.22 | 0.07 | 1.06 |
| 4 | F | 22 | 26 | 1 | CI | 0 | 0 | 0.06 | 0.76 | −0.70 | 0.08 |
| 5 | F | 18 | 18 | 1 | CI | 1 | 0 | 0.06 | 0.60 | −0.54 | 0.10 |
| 6 | F | 27 | 23 | 0 | CI | 0 | 0 | 0.35 | 1.34 | −0.99 | 0.26 |
| 7 | F | 26 | 28 | 1 | CI | 0 | 0 | 0.18 | 0.60 | −0.42 | 0.30 |
| 8 | F | 32 | 27 | 0 | LI | 1 | 1 | 1.09 | 1.35 | −0.26 | 0.80 |
| 9 | F | 25 | 31 | 1 | LI | 0 | 0 | 0.08 | 3.80 | −3.72 | 0.02 |
| 10 | F | 23 | 21 | 0 | LI | 0 | 0 | 0.10 | 2.52 | −2.42 | 0.04 |
| 11 | F | 23 | 35 | 0 | LI | 0 | 0 | 0.10 | 0.90 | −0.80 | 0.11 |
| 12 | M | 22 | 38 | 0 | LI | 0 | 0 | 1.09 | 3.29 | −2.20 | 0.33 |
| 13 | F | 22 | 26 | 1 | LI | 0 | 0 | 0.42 | 0.65 | −0.23 | 0.64 |
| 14 | F | 25 | 31 | 1 | LI | 0 | 0 | 1.82 | 3.43 | −1.61 | 0.53 |
| 15 | F | 27 | 13 | 1 | LI | 0 | 0 | 0.96 | 1.24 | −0.28 | 0.77 |
| 16 | F | 23 | 35 | 0 | CA | 0 | 0 | 0.37 | 0.24 | 0.13 | 1.55 |
| 17 | M | 24 | 20 | 0 | PM | 0 | 0 | 0.01 | 0.17 | −0.16 | 0.07 |
| 18 | F | 20 | 16 | 1 | PM | 0 | 0 | 0.12 | 1.38 | −1.27 | 0.08 |
| 19 | F | 26 | 20 | 0 | PM | 0 | 0 | 0.35 | 3.04 | −2.68 | 0.12 |
| 20 | F | 23 | 35 | 0 | PM | 0 | 0 | 0.30 | 0.63 | −0.32 | 0.48 |
| 21 | F | 27 | 17 | 0 | PM | 0 | 0 | 0.05 | 0.10 | −0.05 | 0.54 |
| 22 | M | 26 | 51 | 0 | PM | 1 | 1 | 1.34 | 1.82 | −0.48 | 0.73 |
| 23 | M | 27 | 36 | 1 | MO | 0 | 0 | 0.11 | 4.53 | −4.42 | 0.02 |
| 24 | F | 25 | 16 | 1 | MO | 0 | 0 | 0.11 | 2.93 | −2.81 | 0.04 |
| 25 | F | 38 | 32 | 1 | MO | 0 | 0 | 0.27 | 2.36 | −2.09 | 0.11 |
| 26 | M | 21 | 24 | 0 | MO | 0 | 0 | 0.11 | 0.42 | −0.31 | 0.27 |
| 27 | M | 24 | 20 | 0 | MO | 0 | 0 | 0.06 | 0.19 | −0.14 | 0.30 |
| 28 | F | 35 | 36 | 0 | MO | 0 | 0 | 0.30 | 0.90 | −0.61 | 0.33 |
| 29 | F | 20 | 16 | 1 | MO | 1 | 1 | 0.12 | 0.25 | −0.13 | 0.48 |
| 30 | F | 38 | 32 | 1 | MO | 0 | 0 | 0.60 | 1.13 | −0.54 | 0.53 |
| 31 | F | 19 | 30 | 0 | MO | 0 | 0 | 0.07 | 0.11 | −0.04 | 0.67 |
| 32 | F | 26 | 16 | 0 | MO | 0 | 0 | 1.34 | 1.82 | −0.48 | 0.73 |
| 33 | M | 24 | 20 | 0 | MO | 0 | 0 | 0.15 | 0.80 | −0.65 | 0.18 |
| 34 | F | 23 | 35 | 0 | MO | 0 | 0 | 1.77 | 1.54 | 0.23 | 1.15 |
| 35 | F | 27 | 17 | 0 | MO | 1 | 1 | 0.04 | 0.03 | 0.01 | 1.43 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


