Introduction
The purpose of this study was to evaluate the efficiency of corticotomy-facilitated orthodontics and piezocision in rapid canine retraction.
Methods
The sample consisted of 20 patients (15-25 years old) with Class II Division 1 malocclusions. The suggested treatment plan was extraction of the maxillary first premolars with subsequent canine retraction. The sample was divided into 2 equal groups. In the first group, 1 side of the maxillary arch was randomly chosen for treatment with corticotomy, and in the second group, piezocision treatment was used. The contralateral sides of both groups served as the controls. Cuts and perforations were performed with a piezotome, and canine retraction was initiated bilaterally in both groups with closed-coil nickel-titanium springs that applied 150 g of force on each side. The following variables were examined over a 3-month follow-up period: rate of canine crown tip, molar anchorage loss, canine rotation, canine inclination, canine root resorption, plaque index, gingival index, probing depth, attachment level, and gingival recession. The rate of canine crown tip was assessed every 2 weeks after the start of canine retraction at 6 time points.
Results
The rates of canine crown tip were greater in the experimental sides than in the control sides in both groups. Corticotomies produced greater rates of canine movement than did piezocision at 4 time points. Canine root resorption was greater in the control sides. The remaining studied variables exhibited no differences between the control and the experimental sides.
Conclusions
Corticotomy-facilitated orthodontics and piezocision are efficient treatment modalities for accelerating canine retraction.
Highlights
- •
Two surgical techniques—corticotomy and piezocision—for accelerating canine retraction were evaluated.
- •
Half of the patients had corticotomy on 1 side, and the other half had piezocision on 1 side.
- •
The other sides in both groups were the controls.
- •
The rates of canine retraction were higher in the surgery side and with corticotomy more than piezocision.
- •
The surgeries had no side effects with regard to the periodontium and type of tooth movement.
The long duration of orthodontic treatment is one of the most frequent complaints of orthodontic patients; it results from the use of traditional mechanical forces to induce movement by stimulation of resorption modeling in the paradental tissues. Recently, it has been claimed that mechanical force is not the only stimulus that can induce tooth movement. The use of pharmaceutical, electromagnetic, laser, and surgical stimuli to accelerate orthodontic tooth movement has attracted considerable scientific interest. Over the years, several surgical techniques have been developed to reduce the overall treatment time. Thus, the use of supplemental dentoalveolar surgeries to accelerate tooth movement has been recommended.
Distal canine movement is the core time-consuming procedure for premolar extraction patients. Conventional techniques result in canine retraction rates of 0.5 to 1 mm per month, depending on the patient’s age and sex. Therefore, full canine retraction can require 5 to 9 months. Conventional treatments with fixed appliances are likely to require 1.5 to 2 years.
For rapid canine retraction, Liou and Huang proposed periodontal ligament distraction. Some researchers have reported the use of dentoalveolar distraction based on the principles of distraction osteogenesis ; others have used selective alveolar decortication and claimed that this procedure invokes transient osteopenia. Modified surgical techniques have been reported to be effective in reducing clinical orthodontic treatment times.
Corticotomy or decortication simply refers to the intentional cutting of cortical bone. The technique has been claimed to dramatically reduce the treatment time because the resistance of the dense cortical bone to orthodontic tooth movement is eliminated. This decreased resistance has been explained by the underlying regional acceleratory phenomenon (RAP) that occurs after a wound; RAP involves the recruitment of osteoclasts and osteoblasts to the injured site for wound healing, which leads to a transient localized demineralization-remineralization phenomenon in the bony alveolar housing.
Moreover, it has been stated that corticotomy-facilitated orthodontics decreases the undesirable adverse effects of orthodontic treatment including root resorption and periodontal damage. The combination of augmentation grafting with corticotomy increases alveolar volume, which results in significantly more attached gingiva and aids the repair of alveolar cortical bone fenestrations and dehiscences. The grafting increases the scope of orthodontic tooth movement because it enables greater tooth movement into stable positions. The main drawback of corticotomy is its minimal acceptance by patients because of the aggressiveness of these procedures, which increase postoperative discomfort and the risk of complications.
Corticision was introduced as a supplemental dentoalveolar surgery in orthodontic therapy to achieve accelerated tooth movement with minimal surgical intervention. Park et al, followed by Kim et al, introduced the corticision technique as a minimally invasive alternative to the creation of surgical injuries to the bone that do not involve flap reflection. In this technique, the authors used a reinforced scalpel and a mallet to pass through the gingiva and cortical bone without raising a flap.
Thereafter, a piezosurgical knife was used to spare the patient the stressful procedure of malletting; this corticision procedure was termed “piezocision.” Piezocision is a new minimally invasive procedure in which a microsurgical blade is used to make gingival microincisions, and piezoelectric incisions of the cortical alveolar bone are then made with an ultrasonic piezosurgical knife. This procedure has recently been reported to be safe and effective in osseous surgeries, such as preprosthetic surgery, alveolar crest expansion, and sinus grafting.
Compared with conventional burs, the use of a piezoelectric knife enhances bone healing without causing osteonecrotic damage and facilitates the preservation of root integrity because of its precise, selective cutting action. Furthermore, because the piezoelectric knife works only on mineralized tissues, it spares the soft tissues and their blood supplies. Hard tissue or soft tissue grafting can be combined with piezocision via selective tunneling, which allows for the correction of gingival recessions and bone deficiencies. This procedure is not feasible with corticision. Piezocision has successfully been used for the rapid treatment of Class II and Class III patients and has been combined with lingual orthodontics and the Invisalign system to achieve both esthetic and rapid treatment.
Because few studies have addressed the effects of corticotomy and piezocision on canine retraction, this study was performed to investigate the potentials of corticotomy and piezocision to accelerate canine retraction and to compare these 2 techniques to determine whether corticotomy can be replaced with the less-invasive piezocision. We also aimed to determine the types of canine movement and any adverse effects that are associated with these 2 techniques. The study was designed to test the null hypothesis that the rates of canine retraction elicited by the conventional method, corticotomy, and piezocision are the same.
Material and methods
This study had approval from the ethical committee of the faculty of dentistry of Ain Shams University, Cairo, Egypt.
The sample consisted of 20 patients with full complements of permanent teeth that necessitated maxillary first premolar extractions and subsequent canine retractions. All patients fulfilled the following criteria: age, 15 to 25 years; Class II Division 1 malocclusion with mild or no crowding; no previous orthodontic treatment; no systemic disease that might have affected bone formation or density, such as osteoporosis, hyperparathyroidism, or vitamin D deficiency; adequate oral hygiene; probing depth values not exceeding 3 mm across the entire dentition; adequate thickness of the attached gingiva (1-2 mm); and no radiographic evidence of bone loss. The patients were equally and randomly divided into 2 groups: a corticotomy group in which corticotomy was randomly assigned to 1 side of the maxillary arch (experimental side), and a piezocision group in which piezocision was randomly assigned to 1 side of the maxillary arch (experimental side). The randomization was performed with coin tosses to prevent selection bias. The sides contralateral to the procedures served as the controls in both groups.
The initial phase of leveling and alignment was first completed with a straight wire 0.022-in slot Roth appliance. On the day before the surgery, 1 maxillary premolar was randomly selected and extracted, and the other premolar was extracted on the day of the surgery; this procedure was implemented to spare the patient the stress of having 2 bleeding sites at the same time and the discomfort of a prolonged procedure.
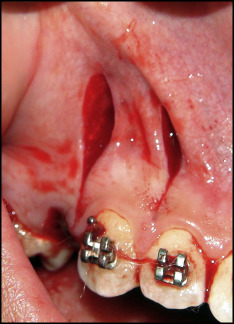
Corticotomy entails flap reflection followed by cuts and perforations in the cortical bone. To preserve the papillae, a submarginal flap was used, where the incision was performed 4 mm apical to the free gingival margin. A number 15 blade in a Bard Parker blade handle (Paragon, Sheffield, United Kingdom) was used to make a buccal incision that followed the contours of the gingiva and extended from the mesial surface of the maxillary lateral incisor to the mesial surface of the maxillary second premolar. A vertical releasing incision was then made, and a full-thickness mucoperiosteal flap was elevated via a mucoperiosteal elevator; this flap was extended beyond the apex of the canine. Using a piezotome (VarioSurg3; NSK, Tokyo, Japan) ( Fig 1 ), bone activation was accomplished with vertical cuts and perforations. The vertical cuts were made along the mesial and distal aspects of the canine root starting 2 to 3 mm below the alveolar crest to protect the crestal bone, and the perforations were made facially along the length of the canine root ( Fig 2 ). The depths of the holes were confirmed by the drop felt when the cancellous bone was reached. The piezotome was used to remove the bundle bone from the mesial wall of the extraction socket of the premolar to decrease the resistance to tooth movement in the desired direction. Thereafter, the flap was repositioned and sutured with nonresorbable 4-0 black silk with the interrupted technique.

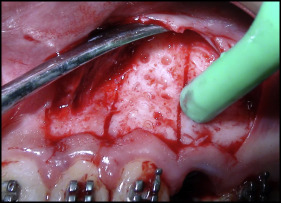
Piezocision involves gingival microincisions and vertical cortical cuts without flap reflection. Interproximal incisions were made through the gingiva on the mesiobuccal and distobuccal line angles of the canine with a number 15 blade in a Bard Parker blade handle. The incisions were made 2 mm below the papillae to preserve the papillae. With the same piezotome, the cortical alveolar incisions were created interproximally ( Fig 3 ). The surgical injury was made 2 mm short of the alveolar crest to preserve the crestal bone and was then extended to the entire length of the canine root. The piezotome was used to remove the bundle bone from the mesial wall of the extraction socket of the premolar to decrease the resistance to tooth movement in the desired direction. The incisions were then sutured with nonresorbable 4-0 black silk with the interrupted technique.
Based on the assumption that the RAP induced by the buccal corticotomy would readily involve the noncorticotomized palatal side, the surgeries were performed only on the buccal cortical plate of the bone to reduce the operation time and the patients’ postoperative discomfort.
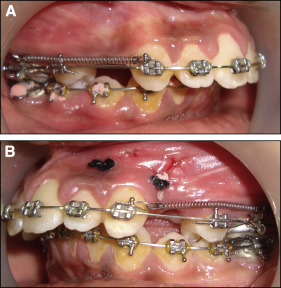
In both groups, a 0.016 × 0.022-in stainless steel wire was tied back immediately after the surgery, and nickel-titanium closed-coil springs that applied 150 g of pressure on each side were used for canine retraction. Canine retraction began immediately after the surgery to take advantage of the RAP induced by bone injury. The coil springs were stretched between the canine and the molar band hooks where the maxillary first permanent molar and second premolar were ligated together and designated as the anchor unit ( Fig 4 ). The retraction force was measured using a strain gauge (Dentaurum, Ispringen, Germany), and the force was calibrated for readjustment at each visit (biweekly). The problem of the transient nature of the RAP was managed by adjusting the orthodontic appliance every 2 weeks to use the continuous mechanical stimulation of the teeth to prolong the osteopenic effect induced by the procedure.
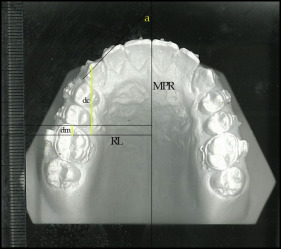
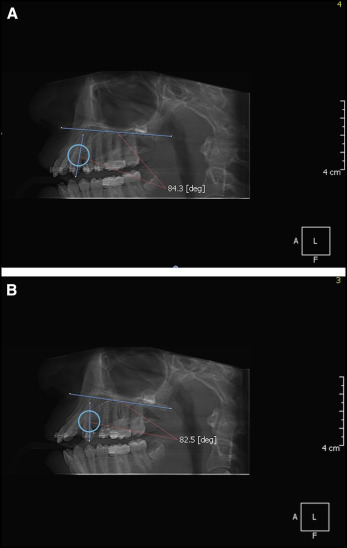
The total follow-up period after the start of the canine retraction was 3 months. Impressions were taken every 2 weeks, and the casts were scanned using a flatbed scanner. The anteroposterior crown tip movements of the canines were assessed at 6 time points (T1-T6) with the method described by Ziegler and Ingervall. The casts were also used to assess the anchorage loss of the first molars and the canine rotation ( Fig 5 ). Cone-beam computed tomography scans taken before and at the end of canine retraction were used to assess the changes in canine inclination and canine root resorption. The angle between the palatal plane and the long axis of the canine was measured before and after canine retraction ( Fig 6 ). Periodontal health was assessed by evaluating the plaque index and the gingival index according to the method of Loe ; moreover, probing depth, attachment level, and gingival recession were recorded.