Introduction
The purpose of this study was to compare the sensitivity of diagnoses of buccal bone coverage in anterior teeth between axial and sagittal reconstructions using cone-beam computed tomography.
Methods
Five dry skulls were clinically evaluated to detect bone defects in the anterior maxilla and mandible to establish a gold standard. The skulls were prepared and placed on a Kodak 9000 3-dimensional scanner (Trophy, Marne La Vallée, France) for image acquisition. The images were processed and reconstructed using Kodak Dental Imaging software 3-dimensional module (version 2.4; Kodak Dental Systems, Atlanta, Ga). All bone defects were identified and recorded.
Results
In the sagittal and axial reconstructions, regions without bone coverage were diagnosed in 91.03% of cases as “cortex not seen” or “minimum thickness, fine, without marrow bone.”
Conclusions
Cone-beam computed tomography can help in the diagnosis of lack of bone coverage on the buccal surfaces of anterior teeth. There was no difference in the performance of the axial and sagittal reconstructions.
Fenestration and dehiscence are bone defects characterized by the absence of alveolar bone coverage, where the root is covered by the periodontal ligament and mucosal lining. They occur in approximately 20% of teeth bilaterally, with greater frequency in the anterior buccal bone.
Diagnosis of the absence of bone coverage is relevant to many areas of dentistry, such as periodontics, prosthetics, surgery, and orthodontics. Exploring the alveolar architecture, the bone support of each tooth, before starting treatment is important for safe planning for each patient. During orthodontic treatment, for example, projection and retraction of the anterior teeth are common. However, the thickness of the alveolar bone on the anterior teeth is a factor that should be considered and measured before and during treatment because the amount of bone in the region can limit tooth movement and the maintenance of periodontal health.
Cone-beam computed tomography (CBCT) imaging has revolutionized maxillofacial diagnostics. CBCT allows micrometric slices to be viewed from selected areas for study. Moreover, improvements in software and workstations have allowed creation of reconstructions from images acquired on various planes, even reconstructions of soft tissues; this facilitates the final diagnosis and explanation to the patient.
In search of knowledge about the contribution of CBCT to bone coverage evaluation and to minimize the deleterious effects of orthodontic therapy, we aimed to detect the absence of bone coverage in the anterior region through axial and sagittal reconstructions by CBCT.
Material and methods
Five dry skulls were selected from the collection of the Department of Orthodontics and Facial Orthopedics at the Professor Édimo Jose Soares Martins Centre at the School of Dentistry of the Federal University of Bahia in Brazil. All skulls were from men between 18 and 25 years of age; they were intact and free of fractures and metallic restorations, with complete dentitions; the teeth had no anomalies.
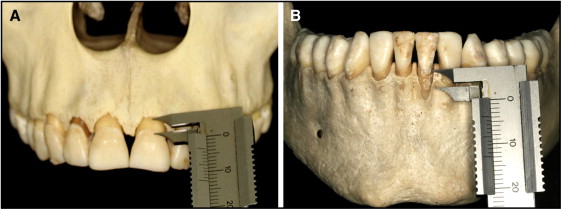
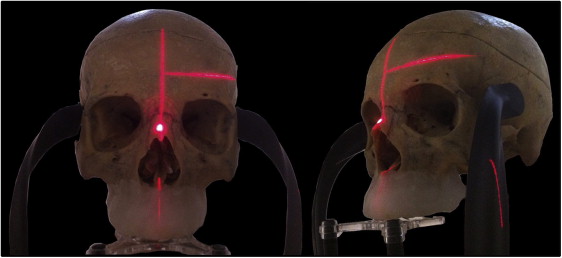
Before image acquisition, the skulls were evaluated by dentists from the orthodontics postgraduate program of Federal University of Bahia to detect any bone defects in the anterior regions of the maxilla and the mandible ( Fig 1 ). With an Odin caliper (Ortho-Pli, Philadelphia, Pa), a lack of bone coverage up to 4 mm was recorded as dehiscence, and a lack of bone marrow along the root of the tooth was classified as bone fenestration. These defects, as well as their locations, were recorded. This clinical evaluation created the gold standard.
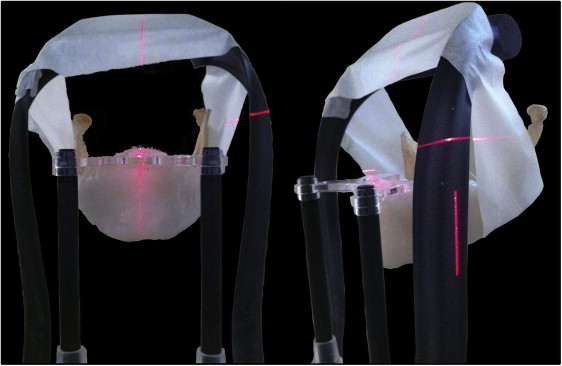
To simulate x-ray attenuation caused by a patient’s soft tissues, the jaws were coated with Wilson utility wax (Polidental, Cotia, Brazil) and then soaked in water for 24 hours before image acquisition ( Fig 2 ).

The skulls and jaws were positioned on a Kodak 9000 3-dimensional unit (Trophy, Marne La Vallée, France) with the median sagittal plane perpendicular to the horizontal plane, and the occlusal plane parallel to the horizontal plane ( Figs 3 and 4 ). For the maxilla, the following image acquisition parameters were used: 60 kV, 8 mA, and 0.2 voxel. For the mandible, the parameters were 60 kV, 6.3 mA, and 0.2 voxel.
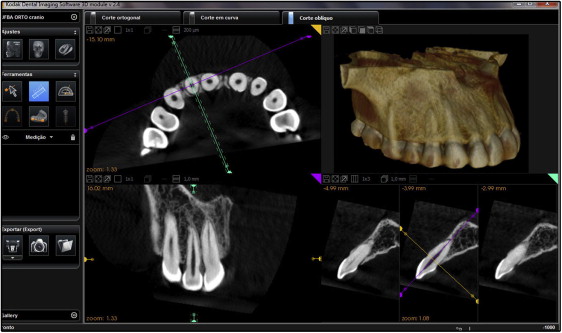
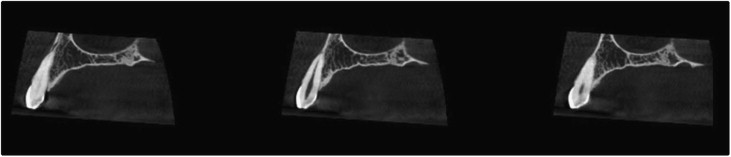
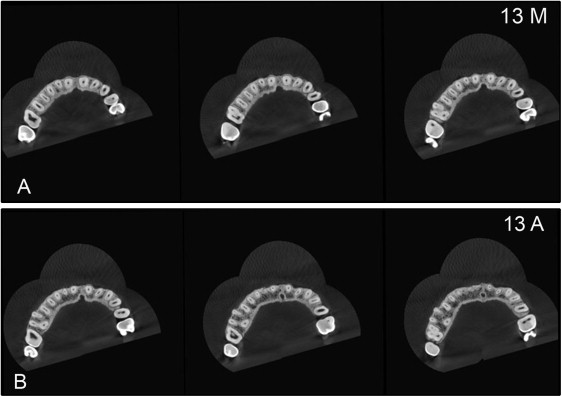
The sagittal images were reconstructed and manipulated using the Kodak Dental Imaging software 3-dimensional module (version 2.4; Kodak Dental Systems, Atlanta, Ga), providing average brightness and contrast. ( Fig 5 ). For each tooth, 3 sagittal reconstructions ( Fig 6 ) and 6 axial reconstructions, 3 from the middle third and 3 from the apical third ( Fig 7 ), were used. The axial reconstructions were prepared in the same way as the sagittal reconstructions, with a thickness of approximately 1.0 mm ( Fig 8 ). All reconstructions were evaluated by 2 radiologists (M.T. and another), with at least 5 years of experience, without knowledge of the study protocol. The examiners evaluated and classified the bone in each third of the tooth using the following criteria: (1) critical: cortex not seen (nonexistent); (2) slender: cortical bone of minimum thickness, thin, without bone marrow; (3) regular: cortical bone and bone marrow visible; and (4) thick: significant amounts of cortical bone and bone marrow.