The primary reasons for splinting and stabilizing teeth are to connect them for the purpose of replacing missing teeth or as an adjunct to periodontal therapy. Although the restorations must be planned to withstand the functional requirements of occlusion and mastication, esthetic considerations must also be taken into account. The challenge in creating an esthetic result with fiber-reinforced composite splints is that there is limited space in the connector region to create the three-dimensional effect required to give teeth the appearance of individuality. Careful planning in the diagnosis and treatment of the fiber splint is essential to allow for adequate tooth preparation to give the illusion of nonsplinted teeth. When missing teeth are replaced with a fiber-reinforced, direct, fixed partial denture, the pontic must be created to achieve an esthetically pleasing result.
Fiber-reinforced composite resins are highly filled composite resins that are strengthened with the use of embedded fiber threads . There are a number of fiber reinforcement materials available for providing dental resin reinforcement in clinical situations ( Table 1 ). Fiber-reinforcement materials can be made from polyethylene yarns woven to create a ribbon, glass fibers woven to create a ribbon, and short and long strands of glass fibers embedded in a resin matrix (preimpregnated glass fibers). In all cases, there are surface treatments of the fibers that allow them to bond to dental resins . Glass fibers are pretreated with organo-silanes that act as chemical coupling agents between dental resin and the glass. Woven fiber ribbons made from high-molecular-weight, high-tensile strength, biocompatible, color-neutral polyethylene are plasma treated. The plasma treatment of the fibers ablates (etches) and chemically activates the fibers to allow them to chemically bond to dental resins, creating a polymeric hybrid that functions as a laminate. The glass and polyethylene fiber reinforcement of the dental resin–fiber network exhibit the characteristics necessary for a load-bearing area even in a thin veneer. In a recent Consensus Conference on fiber reinforcement materials, it was demonstrated that fiber reinforcement materials for composite resins are a highly successful restorative treatment modality and enhance dental care .
| Product (manufacturer) | Type of fiber (widths) |
|---|---|
| everStickC&B, everStickPerio everStick Ortho (Stick Tech, Turku, Finland) | 2 cm preimpregnated glass bundle |
| everStickNet (Stick Tech) | 1 × 30-cm 2 preimpregnated glass fabric sheet |
| Ribbond Reinforcement Ribbon (Ribbond, Seattle, WA) | Lock-stitch, woven polyethylene (1 mm, 2 mm, 3 mm, 4 mm, and 9 mm) |
| Ribbond THM ribbon (Ribbond) | Lock-stitch, woven polyethylene (1 mm ortho, 2 mm, 3 mm, 4 mm, and 7 mm) |
| Ribbond Triaxial (Ribbond) | Three axis braided weave, polyethylene fiber ribbon (dense, thin) |
| Connect (Kerr, Orange, CA) | Open-weave, polyethylene ribbon (2 mm and 3 mm) |
| Splint-It (Pentron, Wallingford, CT) | Open-weave, glass fiber ribbon (2 mm); unidirectional, glass fiber ribbon (3 mm) |
| DVA (Dental Ventures of America, Riverside, CA) | Open tufts of polyethylene fibers |
| GlasSpan rope (GlasSpan, Exton, PA) | Open-weave glass fiber ribbon and (4 mm ribbon, 2 mm, and 3 mm rope) |
Fiber reinforcement within composite resins have a variety of uses that include splinting of teeth , restoration of the endodontically treated tooth , and cross splinting teeth that contain large composite restorations . The most common use for fiber reinforcement that has been described in the dental literature has been the splinting of teeth . A splint, as defined by the Glossary of Prosthodontic Terms , is “a device that maintains hard and/or soft tissue in a predetermined position” . Teeth are splinted for a variety of reasons, including to replace missing teeth, to retain teeth that have been orthodontically repositioned, to stabilize teeth that have been traumatized, and to stabilize teeth that are periodontally involved and have mobility.
When teeth are joined together for the purpose of splinting, stabilization, or restoration as a result of missing teeth, the technical elements of marginal fit, correct contour and shape of the restoration, cleansibility, and occlusion must be fulfilled. In the esthetic zone of the oral cavity, an acceptable cosmetic result must be achieved. Clinically, a splint can be a cast-fixed or removable partial denture or a reinforced adhesive composite resin restoration. A splint joins teeth together with the treatment goal of stabilization, and the connection between the teeth must be strong enough to withstand the forces of mastication and the parafunctional forces of grinding, clenching, and trauma. When anterior teeth are splinted, thorough treatment planning is essential to fulfill the need for a long-term durable restoration without compromising esthetic goals. Therefore, the clinician must design the tooth preparations and subsequent restorations, taking into account the connector areas, interproximal contact areas, incisal/occlusal embrasures, and gingival spaces.
The primary focus of dental care is the treatment of pathologic conditions of the oral hard and soft tissues. The goal of treatment is to establish a physiologically stable result that can be maintained in a healthy state by the patient. At times, treatment results may compromise patient esthetics. How important is the final esthetic result? Lombardi stated that dental esthetics is the most important aspect of all of the dental specialties, including pediatric dentistry, orthodontics, oral surgery, periodontics, and restorative dentistry. He further described physical attractiveness as playing an essential role in one’s self-esteem and as being an important concept for the entire dental team . Dentists have the ability to increase the attractiveness of a patient’s smile, which may change a patient’s life as self-confidence improves. The physiologic implications of esthetic dental treatment to preserve or restore a person’s self-image, self-esteem, and well-being have been well documented . Patients sometimes neglect their oral health until dental disease has a direct impact on their physical appearance. Although a patient’s goal may be to restore the esthetic function of the teeth, this should not compromise overall dental health . It is the dentist’s ultimate responsibility to preserve, enhance, or create a pleasing smile through dental treatment but not at the expense of function. Sometimes the patient’s goal is elimination of dental pain; however, the dentist must not fail to discuss the esthetic implications of a proposed plan of treatment . It is the responsibility of the practitioner to provide a comprehensive treatment plan to the patient, discuss the treatment goals, and strive to attain all treatment goals.
Evaluation of the esthetic zone
The goal patients is that there be a normal esthetic relationship linking the appearance of the teeth, gingival tissues and supporting structures, and the oromaxillofacial complex. From a physiologic standpoint, a smile can be portrayed as a change in the oral musculature that raises the lips at the corners of the mouth into a curve that generally exposes some of the teeth. The amount of tooth structure that can be visualized is dependent on the retraction of the lips from the teeth. In some cases, people expose minimal gingival tissues; however, in other cases, a broad smile reveals all of the gingival tissues. In most cases, when teeth are not splinted together, each tooth has an individualized appearance. Once teeth are joined together through splinting, the connectors change the three-dimensional appearance of the interproximal spaces and the individuality of each tooth.
The esthetic appearance of teeth is a mixture of each individual tooth shape, the position of the teeth within the dental arch, and the interrelationships of the teeth to the opposing dental arch. Depending on tooth position, teeth can create an agreeable or disagreeable visual appearance. The psychologic responses to a person’s smile by others is a blend of complex visual judgments. Within each culture, there are norms regarding what constitutes a pleasing smile. For those who believe their smile is unattractive due to disharmonious tooth position, color, shape, or contours, the oral musculature has been trained to cover the teeth when the person smiles. Even though the lips and corners of the mouth are turning in an upward direction, the teeth are guarded and therefore hidden from view by the oral musculature.
A smile is a combination of the appearance of each tooth, the appearance of the teeth and adjacent gingival tissues as a unit, and how all of these are framed by the oral musculature and lips. In the anterior zone, the maxillary incisors are usually the teeth seen when one smiles. These teeth can have a variety of shapes and forms. Theories of tooth forms and facial profiles led to the description and selection of teeth based upon different tooth forms . From these theories, denture tooth manufacturers classified tooth forms based upon specific descriptions of maxillary incisor shapes. These descriptions include tapering, ovoid, square, square ovoid, and square tapering. Research has shown that there is no correlation between tooth form and facial profile, but these descriptions persist . The basic shape of a tooth is also affected by the facial surface contours, the length and width of the tooth, the position of the facial line angles of the tooth, and the surface texture of the tooth and how it reflects light. Tooth color (shade) is an important facet of the esthetic appearance, especially in this era of tooth whitening. Shades approaching white that were once considered too high in value are now considered normal.
Not only are individual tooth form and color important in the esthetic appearance; how the teeth appear as a group is also important. Within a dental arch, the teeth in the esthetic zone are visualized through the appearance of tooth individualization, tooth arrangement, appearance of each tooth relative to its companion teeth , and the appearance of the gingival tissues . These critical factors include gingival color and contour, midline, tooth size proportion, tooth position, incisal lengths, tooth widths, axial inclination, occlusal plane, and interproximal relationships between teeth.
Healthy gingival tissues have a pleasing appearance and frame the teeth to which they are attached. Gingival tissues that are inflamed and hyperplastic are detractors to a pleasing smile. Healthy gingival tissue adapts to the necks of the teeth and follows the contours of the cementoenamel junction of the teeth and the underlying bone. There is considerable variation in the appearance of gingival tissues relative to tooth position, gingival pigmentation, and thickness of the gingival tissues . In the case of a missing tooth, the gingival shape of the ridge can have a variety of forms due to the reason for tooth loss, the type of surgical procedure required for extraction, or the absence of tooth formation in the ridge area.
Tooth-to-tooth relationships have a direct impact on esthetic appearance. The arrangement of anterior and adjacent teeth in the esthetic zone is the most dominant factor influencing esthetics . In most cases, teeth and smiles are viewed at right angles to the facial surfaces of the maxillary incisors. When one views one’s own teeth, it is generally in a mirror at right angles. The cosmetic appearance of a smile is directly influenced by a society’s expectations for an attractive smile. The most appealing features of a smile as it is framed by the lips and the face are symmetry and proportion . Most people do not have “perfect” symmetry and proportion.
Within the limitations of dental treatment, there are goals that can be accomplished when providing esthetic tooth splinting. An esthetically pleasing appearance can be achieved by having the midline coincide with other centered features of the face (ie, the nose, philtrum, and chin). When splinting teeth, the design of the interproximal connector should be based upon tooth width and length to create a proportional appearance. Splinted teeth are more esthetically pleasing when the incisal edges are aligned without tooth rotations, overlap, or facial or lingual positioning with respect to the arch form. When teeth are splinted, it is important to individualize the appearance of the teeth by creating incisal embrasure spaces without oversilhouetting the light appearance of the teeth against the darker areas of the intraoral cavity .
When viewing the maxillary anterior teeth, the relationship of the occlusal plane to the incisal line of the teeth plays an important role in defining an esthetically pleasing smile. Typically, this is defined by the relationship of the incisal line of the maxillary anterior teeth extending to the facial cusp tips of the posterior teeth. In most cases, the incisal line of the maxillary central incisors should be parallel to the interpupillary line, with the maxillary lateral incisal edges slightly more apical in position, denoting a positive smile line .
In some cases, these “rules” cannot be followed due to the limitations of tooth position, arch space and size, tooth shape and size, and occlusion. During a treatment plan, these limitations need to be explained to the patient. The choice of treatment by the patient may be dictated by their expectation of a desired final result. Major tooth shape, size, color, and alignment issues may be treated best with conventional fixed partial dentures and not fiber-reinforced composites.
Esthetics and splinted teeth
The challenge in creating or maintaining an esthetically pleasing restorative result when splinting teeth is to duplicate those factors that provide an esthetic result when teeth are not joined together. A fixed partial denture is usually the treatment of choice to replace a missing tooth. Frequently, periodontally involved teeth are splinted to control increasing tooth mobility associated with secondary occlusal trauma.
When teeth are joined together with a connector, the result usually produces an artificial esthetic barrier to the three-dimensional appearance of teeth. For a splint to be successful and durable, the connectors between the splinted teeth must have a specific thickness of restorative material to resist fracture in normal function and parafunction. Connectors used for splinting teeth include cast metal, cast metal covered with ceramic, composite resin with embedded fiber ribbon, metal bars or wires, and nylon mesh. Teeth with spacing present an additional esthetic dilemma. If the spaces are to be maintained, the connector used for splinting must be placed so it is not visually apparent.
In most cases, the optimal placement of the interproximal connector from a facial view when splinting is on the incisal/occlusal or middle third of the tooth. This location mimics the presence of the interproximal contact area between adjacent teeth. This location also provides access for the clinician to shape the restoration and reestablish an esthetic result. The management of the incisal/occlusal embrasures, facial interproximal connector areas, and the gingival embrasures is important to achieve desirable esthetics and function. When planning a splint or fixed partial denture, the lingual surfaces of the restored teeth must be designed to have adequate thickness for the bulk of the restorative material to resist the forces of occlusion and mastication. In some cases, it may be necessary to reshape opposing teeth to establish occlusal patterns that allow the connector to have the required thickness for clinical durability.
The placement of the connector in the incisal/occlusal or middle third of the tooth is important in the establishment of an esthetic and hygienic gingival embrasure . The gingival embrasure must be designed so that the patient has access to remove plaque to maintain periodontal health and prevent caries.
The type of splint being planned has a major impact on the final esthetic appearance of the case. In clinical situations where a porcelain–metal or all ceramic restoration is planned, tooth preparations allow for easier and better esthetic and occlusal control of the final result. The esthetic limitations of splinted teeth are minimized with a laboratory-fabricated, fixed partial denture. When a fiber–reinforced, direct composite resin is being placed, the conservation of tooth structure for a predictable bonding surface of enamel requires more complex treatment planning by the clinician to achieve an esthetic final result. It is critical that the clinician observe the esthetic needs of the case in the planning and tooth modification required from several important esthetic dimensions: incisal embrasure form, facial and interproximal embrasure form, and gingival embrasure form. These aspects in planning and restoration are demonstrated through several cases of splinting using fiber reinforcement.
Incisal embrasure form
The incisal embrasures are critical for the esthetic silhouette of the incisal edges of maxillary and mandibular teeth. If each tooth is not individualized by carving this feature into the splint, the teeth have a block-like appearance. This loss of individuality decreases the illusion of spacing. Using tooth contour with the establishment of definitive incisal embrasures improves the facial appearance of the teeth in profile. Designing incisal embrasures outlines the difference in heights and separation of the maxillary incisal edges and differentiates each mandibular incisor as a separate entity. Otherwise, the teeth appear as one solid block without distinction between each tooth. In the maxillary arch, the incisal embrasure between the central incisors is in most cases approximately 1.0 mm lower than the embrasures between the central and lateral incisors. The incisal embrasure between the lateral incisor and canine is generally longer because of the change in shape between the more square or tapered lateral incisor and the more triangular incisal appearance of the canine. The embrasure form of the mandibular incisors, although not as prominent as the maxillary incisors, is just as important in creating a natural visual impact through incisal separation . As we get older and the incisal edges wear, the incisal embrasure decreases and eventually can vanish, leaving the block-like appearance .
With these factors in mind, the design of the restoration has to allow for adequate incisal embrasure without compromising strength and durability in the connector of the restoration. For cast porcelain–metal and all-ceramic restorations, the tooth preparation must allow for the design of the framework so that final porcelain application can be accomplished, allowing each tooth to be distinct from the adjacent teeth. The final crown preparation must take this into account so that the framework in the incisal area of the connector allows for at least 1.0 to 1.2 mm of porcelain covering the metal or ceramic substructure. For reinforced, bonded composite resin splints, the reinforcement ribbon must be placed so that at least 1.0 mm of composite resin remains after esthetic carving of the incisal embrasure form. Less thickness of the composite resin can lead to premature fracture and exposure of the fibers. Shaping should be accomplished, creating incisal embrasure form from the lingual and facial surfaces so that the final tooth form from an incisal view is maintained.
Facial and interproximal form
The three-dimensional illusion of the teeth within a splinted restoration is achieved by careful design of the tooth preparations. In the case of porcelain–metal or all-ceramic restorations, the tooth reduction creates the room for the overlying metal or ceramic substructure with the esthetic porcelain applied. Typical crown preparations easily allow for these requirements for the final restoration. For conservative fiber-reinforced splinted restorations, there are limitations to the amount of tooth structure that can be prepared based upon the tooth substrate to be bonded to (preferably enamel) and the existing occlusion. Evaluation of occlusion to fulfill the requirements of the fiber-reinforced composite must be done in maximum intercuspation and in excursive movements. If interferences are created when the definitive restoration is fabricated, the teeth must be modified by preparation to eliminate the potential for these interferences. This must be done as part of the diagnosis and treatment planning phase using casts mounted on an articulator.
After a comprehensive evaluation, decisions must be made on how the tooth shapes need to be modified and prepared to allow for an esthetic interproximal and facial embrasure form that does not compromise the durability of the definite fiber-reinforced splint. In contrast to porcelain–metal and all-ceramic fixed partial denture splints, composite resin restorations are more susceptible to fatigue failure. By using reinforcement materials embedded within the composite, such as woven polyethylene ribbon or unidirectional glass fibers, the potential fracture and separation of the splint can be overcome . When reinforcement ribbon and composite resin is used for splinting, the physical properties of the laminated structure can be maximized by placing the ribbon in the tensile zone of the splint .
For maxillary periodontal splints, definitive tooth preparation of the facial surface to compensate for thickness of fiber ribbon reinforcement and composite is necessary to eliminate the overcontouring of the final restoration. Facial placement of the fiber also allows for maintaining occlusion on tooth rather than composite . In the case of a periodontal splint, there is concern that the patient will wear the lingual surface of the composite resin into the fiber reinforcement, leaving the fibers exposed and compromising the durability of the splint. For cases of direct single-tooth replacement with a fiber-reinforced, composite, fixed partial denture for the maxillary arch, the use of Class 3 preparations on the adjacent abutment teeth and a lingual channel with adequate depth to place the fiber closer to the facial surface and the tensile zone is necessary.
To achieve facial and interproximal individualization of teeth, it is necessary that tooth preparation for maxillary and mandibular fiber splints barrel into one half of the interproximal contact area using a medium-grit diamond on the high-speed handpiece. This facial preparation minimizes bulk on the esthetic facial surface interproximally and allows the composite resin to have adequate thickness for strength while allowing it to be shaped for esthetic individualization of each tooth that is splinted. Other purposes for the placement of facial composite resin are to seal the interproximal areas against recurrent caries, to provide for a 180° wrap of composite resin to each of the splinted teeth, and to stabilize the teeth to prevent movement when the composite resin and ribbon are placed onto the lingual surface for mandibular splints. For maxillary periodontal splints, some additional interproximal preparation is necessary so that the fiber reinforcement material can be pushed and embedded within the interproximal contact area, allowing for room to shape an esthetic composite resin in the connector area. This facial extension of composite resin also functions as a cross-splint for each tooth to prevent tooth movement and breakage of the final splint.
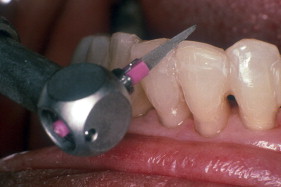
When the fiber-reinforced composite resin is light cured, shaping and individualization of each tooth in the connector area can be accomplished with ultrathin, needle-shaped diamonds with a high-speed handpiece; with thin disks with a slow-speed handpiece; or with a reciprocating handpiece (Profin; Dentatus, New York, NY) with thin, flat, safe-sided, diamond-impregnated Lamineer tips ( Fig. 1 ). The experience of these authors is that the reciprocating handpiece is less problematic in forming these facial embrasure areas because of its precision for fine shaping in these areas.
Gingival form
Just as important as tooth form and individuality of the facial interproximal areas at the connectors and the incisal embrasure form is the gingival embrasure. When designing a splinted restoration, the gingival embrasure form must allow for maintenance of gingival health. The pink-stippled gingival appearance contributes to the overall esthetic appearance of the restoration. If the patient cannot maintain the gingiva with oral hygiene procedures, the gingiva can develop an erythematous, edematous appearance that detracts from the esthetic appearance of the final restoration.
In the case of the replacement of a long-standing missing tooth in the esthetic zone, the pontic shape should have a light contact on the ridge. Recontouring the gingival ridge to create an ovate pontic emerging from the ridge is recommended . This emergence profile of the pontic should mimic the contours of the adjacent teeth. Another significant gingival esthetic problem is the presence of a localized defect on the ridge. Before fabrication of the definitive fixed partial denture to replace the missing tooth or teeth, a surgical technique similar to that used in root coverage procedures using a soft connective tissue graft to eliminate the defect has been successful . Also, the facial form of the pontic must match the analogous tooth in the arch in shape and size and disguise the interdental space. The physical requirements of the connector must also be taken into account.
In many cases, the use of a direct-placement, fiber-reinforced, fixed partial denture is recommended for sudden tooth loss in the esthetic zone of the anterior region usually due to trauma, periodontal disease, or endodontic failure. The use of fiber-reinforced composites for periodontal splinting creates an esthetic challenge in the management of the gingival embrasure area. For the replacement due to sudden loss of an anterior tooth, the pontic can be fabricated using the patient’s own tooth, an acrylic denture tooth, or a tooth made from composite resin . The placement of the pontic slightly within the healing socket can create an esthetically emerging pontic when the socket heals. It is important that the tooth pontic be slightly longer for placement slightly within the healing socket.
When completing the finishing and polishing of the fiber splint, careful attention should be given to shaping the gingival embrasure interproximal areas. If there is an excess of composite resin in the gingival embrasure spaces, a Profin reciprocating handpiece with a flat Lamineer tip can be used to finish those areas. The reciprocating handpiece is used because access to the gingival margins on the proximal surfaces is limited when teeth are splinted. Finishing strips do not work well on rounded or concave root and interproximal surfaces. Likewise, the use of rotary handpieces with rotating finishing diamonds and burs often used in these interproximal areas is contraindicated because they can create unnatural embrasures and notched irregular surfaces. The reciprocating handpiece, with its back-and-forth reciprocating motion, can be used to remove excess resin and finish the gingivo-interproximal surfaces to natural form ( Fig. 2 ). The final shaping of the gingival embrasure must permit the gingival tissues of the papilla to form a collum and adapt to the gingival areas of the tooth crown.



