An adolescent boy with an Angle Class II Division 1 malocclusion had a hyperdivergent growth pattern with an excessive lower facial height and an anterior open bite. Combined orthodontic and surgical treatment should be considered for patients with a skeletal anterior open-bite malocclusion. For patients who do not want surgery, however, a 0.022 × 0.028-in nontorqued, nonangulated fixed appliance with a chincup as adjunct therapy is an alternative that can have excellent results. The final outcome of this treatment were great improvements in function, esthetics, and posttreatment stability after 8 years.
Skeletal anterior open bite is a complex and multifactorial anomaly, and it is considered to be one of the most difficult orthodontic problems to correct. Proper diagnosis, successful treatment, and long-term retention of open-bite malocclusions have been frequent topics of discussion and research studies.
Previous studies with lateral cephalometric radiographs showed that skeletal open bites are characterized by a steep mandibular plane, an obtuse gonial angle, and increased height of the lower third of the face. In adults, treatment of severe skeletal anterior open bite consists mainly of surgically repositioning the maxilla or the mandible. It has been shown that skeletal anchorage, such as microscrew implants, can produce treatment outcomes that can only be obtained from orthognathic surgery, not from conventional orthodontic treatment.
Many patients do not readily accept orthognathic surgery. For this reason, orthodontic correction of morphologic and functional problems affecting the patient’s psychology at an early stage can help eliminate potential inferiority complexes and have a beneficial effect on personality development.
In a nonsurgical plan, the orthodontist camouflages the skeletal discrepancies to satisfy as many of the patient’s esthetic and functional concerns as possible. In such treatments, the patient must be informed about the complexity of the plan and the need for perfect compliance.
This case report illustrates the successful treatment and the 8-year posttreatment stability of a severe skeletal open bite in a patient with a hyperdivergent growth pattern.
Diagnosis and etiology
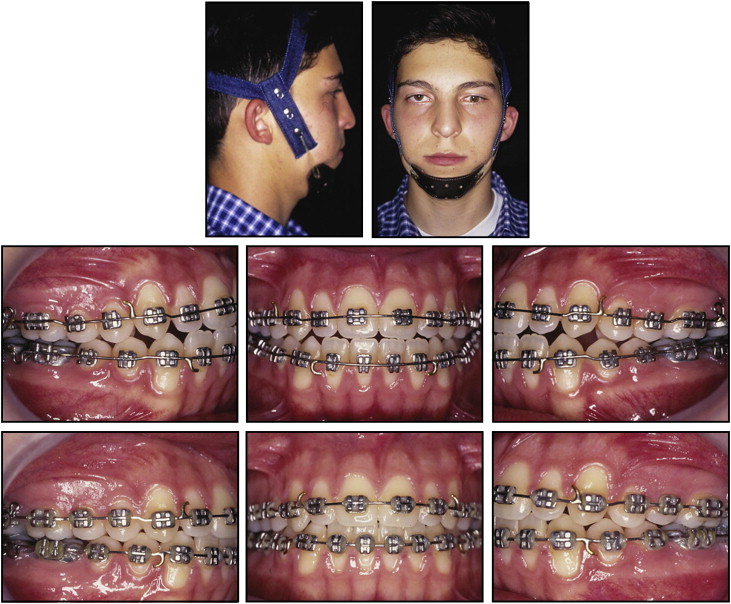
The patient was a 13-year-old boy with an anterior open bite. According to the interview, his father had mandibular prognathism. The pretreatment facial photographs ( Fig 1 ) show a convex profile with increased lower anterior facial height and unstrained lip closure. The patient had dental biprotrusion, with the left second premolar in crossbite and a 6-mm anterior open bite. The intraoral view also shows the malpositioned tongue resting between the incisors. This tongue posture might have played a role in establishing the malocclusion. The patient had a tongue-thrust swallow and atypical phonation as physiologic adaptations to the open bite.

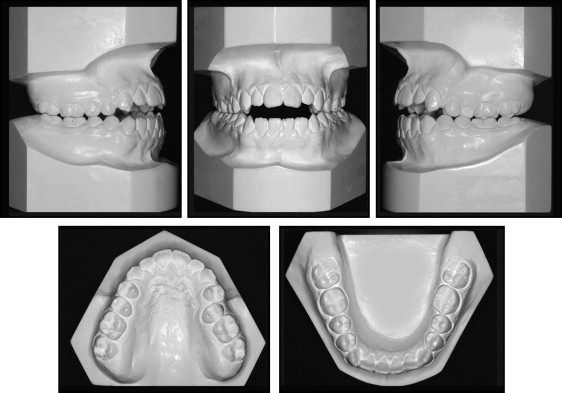
He had an Angle Class II Division 1 malocclusion ( Fig 2 ). The mandibular arch had good shape, no crowding, and a proper curve of Spee. The maxillary arch had overeruption of the posterior teeth and a significant step between the anterior and posterior segments. The pretreatment panoramic radiograph ( Fig 3 ) showed healthy teeth and periodontium.
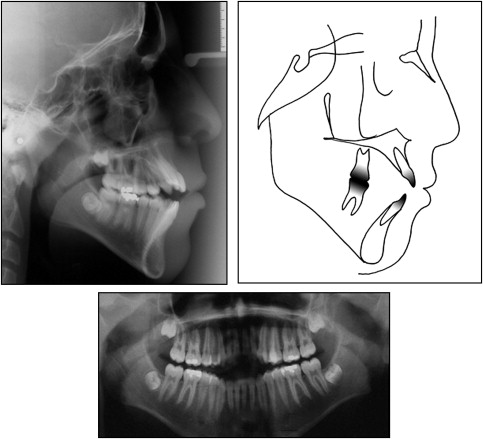
Most of these facial and dental aspects contributed to the patient’s low self-esteem and high introspection. Cephalometric analysis showed a Class I skeletal pattern with a vertical growth pattern. The incisors were proclined, and the axial inclination was increased ( Table ).
| Measurement | Pretreatment | Postreatment | 8-year retention |
|---|---|---|---|
| SNA angle (°) | 75 | 76 | 77 |
| SNB angle (°) | 73 | 74 | 74 |
| ANB angle (°) | 2 | 2 | 3 |
| SND angle (°) | 70 | 71 | 71 |
| 1-NA (mm) | 10 | 8.5 | 7.5 |
| 1-NA (°) | 33 | 28 | 27 |
| 1-NB (mm) | 8.5 | 8 | 9 |
| 1-NB (°) | 30 | 25 | 25 |
| Interincisal angle (°) | 115 | 125 | 125 |
| GoGn-SN) (°) | 45 | 44 | 44 |
| Y-axis (°) | 69 | 71 | 68 |
| SN.occlusal plane | 19 | 16 | 18 |
| Facial angle (°) | 80 | 79 | 82 |
| SN.palatal plane (°) | 6 | 7 | 8 |
| AO-BO (mm) | −1 | 1 | 1 |
Treatment objectives
The treatment objectives were to (1) control vertical growth so that the mandible would rotate in an upward and forward direction, (2) prevent extrusion of the molars by maintaining or diminishing the mandibular plane angle, (3) improve the position of the incisors, (4) correct the open bite by normalizing the overjet and overbite relationships, (5) correct the crossbite on the left second premolar, (6) establish functional occlusion, and (7) improve the vertical proportional balance of the facial thirds and, consequently, the patient’s self-esteem.
Treatment objectives
The treatment objectives were to (1) control vertical growth so that the mandible would rotate in an upward and forward direction, (2) prevent extrusion of the molars by maintaining or diminishing the mandibular plane angle, (3) improve the position of the incisors, (4) correct the open bite by normalizing the overjet and overbite relationships, (5) correct the crossbite on the left second premolar, (6) establish functional occlusion, and (7) improve the vertical proportional balance of the facial thirds and, consequently, the patient’s self-esteem.
Treatment alternatives
Based on the skeletal discrepancies, a combination of orthodontic and orthognathic surgical treatment was suggested, but the family refused. Temporary anchorage devices would have been used to intrude the maxillary and mandibular posterior teeth; however, minimal evidence regarding their efficiency was available. Extraction of the maxillary and mandibular first premolars was considered, but this would have had a negative effect on the facial profile.
A nonextraction orthodontic approach with a high-pull chincup was started after evaluation of the patient’s compliance with prolonged use of extraoral forces. Stabilizing or decreasing the backward and downward mandibular rotation tendency is mandatory for obtaining a successful result in open-bite treatment.
Treatment progress
The first step involved the use of the high-pull chincup to control the vertical growth, and a force of 350 g was applied to each side for 16 to 18 hours per day. After 3 months of chincup therapy, the patient was stabilized, and a standard fixed edgewise appliance with 0.022 × 0.028-in slots was attached. Leveling and alignment of the maxillary and mandibular arches were achieved with 0.014-in to 0.020-in archwires. The maxillary and mandibular archwires had steps (occlusal toward anterior) between the lateral incisors and the canines, and between the second premolars and the first molars. The archwires combined with the intensive vertical force from continued therapy with the high-pull chincup improved the open-bite mechanics.
After a year of comprehensive orthodontic treatment, the horizontal plane divergence decreased minimally. Cephalometric superposition exhibited great control of the subsequent vertical growth as the horizontal planes stabilized or rotated counterclockwise.
Although both arches were leveled and aligned, the overbite was still negative, and the cusp-to-cusp relationship was end to end. This situation confirmed a Bolton discrepancy, as evidenced in the previous dental-cast analyses. Interproximal stripping (4.0 mm) of the mandibular incisors was performed with diamond burs, and hooks were soldered to the maxillary and mandibular 0.020-in stainless steel archwires for Class III intermaxillary elastic mechanics.
After 24 months of comprehensive treatment, the chincup therapy was reduced to night use only, and 0.019 × 0.026-in stainless steel archwires, maintaining the same steps and hooks, were placed. Class III intermaxillary elastics mechanics were maintained ( Fig 4 ). After almost a year, finalizing interproximal stripping (1.0 mm) combined with vertical elastics improved the occlusal interdigitation.