This case report demonstrates the efficient use of implant anchorage in a patient with mesially inclined mandibular molars and an overerupted maxillary molar. A 14-year-old girl had an overerupted maxillary right first molar, possibly because of severely inclined mandibular right molars. Two-step use of miniplate anchorage in the right zygomatic process was proposed. As the first step, the overerupted maxillary first molar was intruded with elastic chains from the miniplate for 10 months. Then the maxillary right molars were distalized by using the miniplate to correct the Class II molar relationship. In the mandible, the first molar was extruded with intermaxillary elastics applied from the miniplate to the molar for 7 months after the uprighting of the mandibular right second molar. The results suggest that the use of 2-step implant anchorage is efficient for intrusion and distalization of maxillary molars and extrusion and uprighting of mandibular inclined molars.
Infraocclusion or missing teeth often cause mesial tipping of adjacent or opposing teeth, and it is frequently observed in the mandibular posterior region. Mandibular mesially inclined teeth become a problem not only in the mandible, but also in the maxilla with overeruption of opposing teeth. As a result of these processes, the occlusal plane becomes canted, and occlusal interferences might be produced. Orthodontic treatment to correct the overerupted molar is recommended before uprighting the mandibular teeth. However, real intrusion is considered extremely difficult with conventional orthodontic mechanics, because of insufficient anchorage.
Recently, bone-anchored orthodontics has become a new treatment strategy. Titanium miniplates or miniscrews placed in bone provide absolute anchorage for various tooth movements without patient cooperation. Additionally, bone-anchored tooth movement does not induce reciprocal movement of other teeth. Recently, successful maxillary molar intrusion has been reported with implant anchorage. Furthermore, maxillary molars have also been moved distally by using bone-anchored orthodontics.
In conventional orthodontic mechanics, several methods have been proposed for uprighting inclined mandibular molars: eg, upright spring, lingual arch appliance, and multi-bracket appliance with high-pull J-hook headgear or Class III elastics. In addition, the use of implant anchorage has already been reported for molar uprighting. However, most reports describe the uprighting of mandibular second molars, and there are few reports using implant anchorage to upright severely inclined mandibular first and second molars.
This case report demonstrates the usefulness of implant anchorage in a patient with mesially inclined mandibular first and second molars and the compensatory overeruption of the maxillary first molar.
Diagnosis and etiology
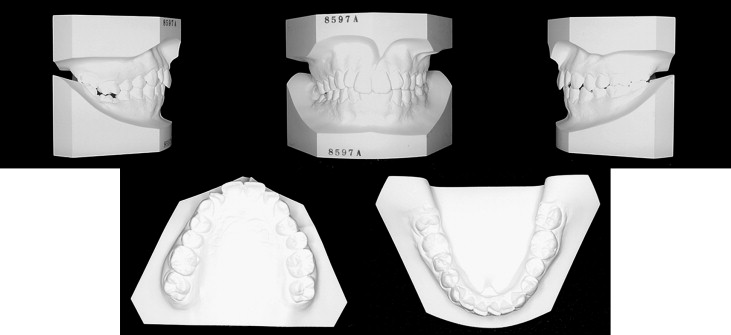
The patient was 14 years 1 month old when she came with an overerupted maxillary right molar and mesially inclined mandibular right molars ( Fig 1 ). She complained about difficulty chewing because of the mesial inclination of the mandibular right molars. Her facial profile was straight with adequate lip prominence compared with the esthetic line and no facial asymmetry. Overjet and overbite were +3.0 and +2.5 mm, respectively. The molar relationships were Class II on the right side and Class I on the left side ( Fig 2 ). The maxillary right first molar was overerupted, and the mandibular right first molar was infraoccluded. The intraoral radiograph showed cemental hyperplasia of the mandibular right first molar without clear delineation of the lamina dura ( Fig 3 ). The mandibular right second molar was significantly inclined. There was moderate incisor crowding in both arches. The arch length discrepancies were –4.5 mm in the maxilla and –4.0 mm in the mandible. The maxillary dental midline was deviated 1.0 mm, and the mandibular midline was 2.0 mm to the right of the facial midline. Periodontal problems and temporomandibular joint disorders were not found.
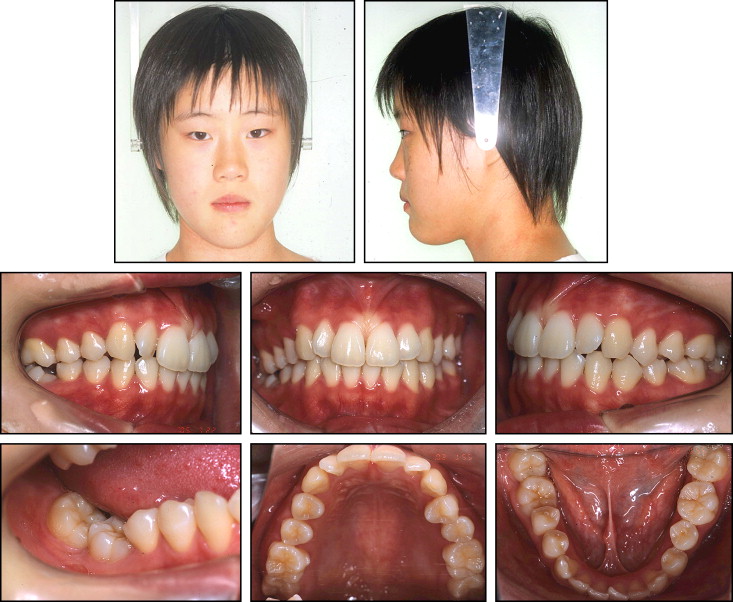
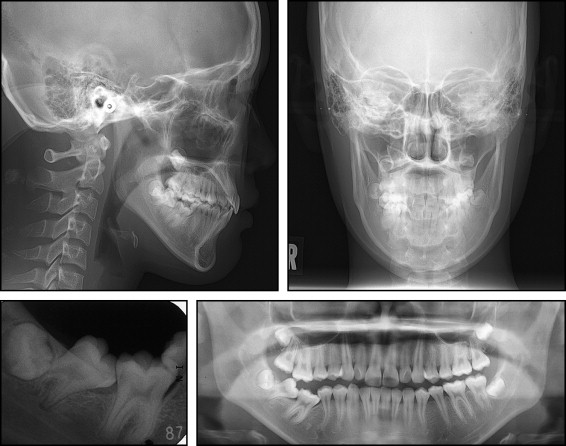
Cephalometric analysis indicated a skeletal Class I relationship (ANB, 3.9°) ( Table ). The mandibular plane angle was within the normal range, but the gonial angle was larger than the Japanese norm (MP/FH, 31.1°; gonial angle, 131.5°). The mandibular body length was within the normal range. Although the maxillary incisors showed a normal labiolingual inclination, the mandibular incisors were tipped more lingually (IMPA, 82.8°). The maxillary right first molar was significantly extruded (U6/PP, 28.0 mm), but the mandibular right first molar was intruded (L6/MP, 29.0 mm).
| Variable | Japanese norm | SD | Pretreatment | Posttreatment |
|---|---|---|---|---|
| Angular (°) | ||||
| ANB | 2.8 | 2.4 | 3.9 | 3.7 |
| SNA | 80.8 | 3.6 | 79.4 | 79.4 |
| SNB | 77.9 | 4.5 | 75.5 | 75.7 |
| MP-FH | 30.5 | 3.6 | 31.1 | 30.6 |
| Gonial angle | 122.1 | 5.3 | 131.5 | 130.0 |
| U1-FH | 112.3 | 8.3 | 111.1 | 114.8 |
| L1-MP | 93.4 | 6.8 | 82.8 | 85.9 |
| Interincisal angle | 123.6 | 10.6 | 135.1 | 128.8 |
| Occlusal plane | 16.9 | 4.4 | 0.1 | 6.7 |
| Linear (mm) | ||||
| S-N | 67.9 | 3.7 | 75.0 | 74.9 |
| N-Me | 125.8 | 5.0 | 137.6 | 138.2 |
| Me/NF | 68.6 | 3.7 | 44.5 | 46.5 |
| Ar-Go | 47.3 | 3.3 | 48.7 | 49.7 |
| Ar-Me | 106.6 | 5.7 | 117.0 | 120.0 |
| Go-Me | 71.4 | 4.1 | 77.0 | 77.5 |
| Overjet | 3.1 | 1.1 | 3.0 | 3.0 |
| Overbite | 3.3 | 1.9 | 2.5 | 2.5 |
| U1/PP | 31.0 | 2.3 | 32.5 | 32.3 |
| U6/PP ∗ | 24.6 | 2.0 | 28.9 | 25.8 |
| L1/MP | 44.2 | 2.7 | 47.6 | 47.9 |
| L6/MP ∗ | 32.9 | 2.5 | 29.0 | 32.4 |
Treatment objectives
From these findings, this patient was diagnosed as having moderate crowding with a skeletal Class I jaw-base relationship. The maxillary right first molar was significantly overerupted, and the mandibular second molar was mesially inclined, possibly because of infraocclusion of the mandibular right first molar. The treatment objectives were (1) to correct the molar relationship on the right side, the mesial inclination of the mandibular molars, and the extrusion of the maxillary first molar; (2) to maintain ideal overjet and overbite; and (3) to achieve a functional Class I occlusion.
Treatment objectives
From these findings, this patient was diagnosed as having moderate crowding with a skeletal Class I jaw-base relationship. The maxillary right first molar was significantly overerupted, and the mandibular second molar was mesially inclined, possibly because of infraocclusion of the mandibular right first molar. The treatment objectives were (1) to correct the molar relationship on the right side, the mesial inclination of the mandibular molars, and the extrusion of the maxillary first molar; (2) to maintain ideal overjet and overbite; and (3) to achieve a functional Class I occlusion.
Treatment altervatives
The maxillary first molar was significantly extruded and had a Class II malocclusion on the right side; therefore, we planned to place a titanium miniplate in the right zygomatic process as bone anchorage for maxillary molar intrusion and distalization. Without skeletal anchorage, absolute intrusion of the overerupted molar would be impossible. Maxillary premolar extraction could be considered to treat the Class II malocclusion, but the patient had moderate crowding with an acceptable facial profile and a strong desire to avoid tooth extractions except for the third molars. Therefore, we chose maxillary molar distalization. The molars could be distalized with conventional fixed appliances, but this would require patient cooperation in wearing an extraoral device or intermaxillary elastics to prevent side effects.
Mesial inclination of the mandibular molars on the right side could also be treated by traditional uprighting mechanics including Class III elastics. However, Class III elastics applied to the maxillary molars directly might worsen the Class II intermaxillary relationship and the overerupted maxillary molar in this patient. The mandibular dental midlines were slightly deviated to the right with respect to the facial midline before treatment. Tooth extraction or the use of implant anchorage would be required on the left side in both jaws for midline correction. However, facial asymmetry was not observed, and the midline deviation was considered almost acceptable at the initial examination. Additionally, the patient was not concerned about the midline deviation. She complained only about difficulty in chewing on the right side. Therefore, we did not plan to correct the dental midline deviation.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


