Introduction
In this study, we compared the efficiency of Class II subdivision malocclusion treatment with symmetric and asymmetric extractions.
Methods
A sample of 71 patients with complete Class II subdivision malocclusion was selected: group 1 consisted of 40 patients treated with 4 premolar extractions with an initial mean age of 13.37 years, and group 2 had 31 patients treated with 3 premolar extractions (2 maxillary premolars and 1 mandibular premolar on the Class I side) with an initial mean age of 14.44 years. To compare the efficiency of each treatment protocol, the initial and final occlusal results were evaluated on dental casts with the Peer Assessment Rating occlusal index, and time spent in treatment was calculated from the clinical charts. The amounts of initial and final midline deviation and improvement of midline deviation correction were also evaluated. Efficiency was calculated as the rate between occlusal improvement by the treatment time. The groups were compared with t and Mann-Whitney tests.
Results
The results showed that group 2 had a significantly smaller final amount of midline deviation and a greater correction of midline deviation.
Conclusions
Treatment efficiency of type 1 Class II subdivision malocclusions with 3 or 4 premolar extractions is similar. However, treatment with 3 premolar extractions provides a better occlusal success rate.
Highlights
- •
We compared the efficiency of symmetric and asymmetric extractions in type 1 Class II subdivision malocclusions.
- •
The efficiency of treatment was similar in both groups.
- •
The group treated with asymmetric extractions had a better occlusal success rate.
Class II subdivision malocclusion can be classified in 2 types. Type 1 is characterized by distal positioning of the mandibular first molar on the Class II side—in this type, the maxillary midline is coincident with the midsagittal plane, and the mandibular midline is deviated to the Class II side in a frontal view, Type 2 is characterized by mesial positioning of the maxillary first molar on the Class II side—in this type, the maxillary midline is deviated to the Class I side, and the mandibular midline is coincident with the midsagittal plane. Several investigations have focused on the efficiency of the treatment protocols in the correction of different malocclusions. Efficiency consists in the achievement of the best results in the shortest time. It has already been demonstrated that type 1 Class II subdivision malocclusions treated with 3 premolar extractions have a higher occlusal success rate than treatment with 4 premolar extractions, since obtaining a Class I molar relationship on the Class II malocclusion side in the 4 premolar extraction protocol requires more anchorage reinforcement with removable appliances and patient compliance than maintaining the Class II molar relationship in the 3 premolar extraction protocol on that side. Treatment time is also shorter in the 2 maxillary premolar than in the 4 premolar extraction protocol in complete Class II malocclusion correction, because molar relationship correction, inherent to nonextraction and 4 premolar extraction protocols, is thought to increase the Class II treatment time. Following this rationale, it could be speculated that probably a 3 premolar extraction protocol could also have a shorter treatment time than a 4 premolar extraction protocol in Class II subdivision malocclusion patients. Although the results have been individually compared between treatment protocols in Class II subdivision malocclusions, the amounts of change in a time period have not been related to each other to evaluate the degree of treatment efficiency.
Thus, the purpose of this study was to test the following null hypothesis: “Type 1 Class II subdivision malocclusion treatment efficiency is similar in 4 premolar and 3 premolar extraction protocols.” Therefore, occlusal results, treatment times, and the efficiency index were compared between 2 groups treated with these protocols.
Material and methods
This study was approved by the ethics in research committee of Bauru Dental School at the University of São Paulo in Brazil.
The sample was selected from the files of the Department of Orthodontics at Bauru Dental School, University of São Paulo. Initial and final dental study models of 71 patients who had type 1 Class II subdivision malocclusions (complete Class II on 1 side and Class I on the other side) and were treated with fixed appliances with a 4 or a 3 premolar extraction protocol were selected. The sample was then divided into 2 groups. Group 1 consisted of 40 patients treated with 4 premolar extractions with an initial mean age of 13.37 ± 1.31 years (range, 10.25-15.91 years), and group 2 consisted of 31 patients treated with 3 premolar extractions (2 maxillary premolars and 1 mandibular premolar on the Class I side) with an initial mean age of 14.44 ± 2.83 years (range, 10-24.25 years). The selection criteria were a full Class II molar relationship on 1 side and a Class I molar relationship on the other side, and the presence of all permanent teeth up to the first molars. The additional selection criteria were (1) no previous orthodontic treatment, (2) no history of facial trauma that could have altered growth of the apical bases, and (3) complete orthodontic records. To select the sample, only the initial anteroposterior relationship was considered. No other dentoalveolar or skeletal characteristic was considered.
Orthodontic mechanics included fixed edgewise appliances, with 0.022 × 0.028-in conventional brackets and the usual wire sequence characterized by an initial 0.015-in twist flex or a 0.016-in nickel-titanium alloy archwire, followed by 0.016, 0.018, 0.020, and 0.021 × 0.025 or 0.018 × 0.025-in stainless steel archwires (3M Unitek, Monrovia, Calif). Accentuated and reverse curve of Spee were used to correct the deepbites. Rectangular wires and elastic chains were used for en-masse retraction and to correct overjet and Class II canine relationship. Extraoral headgear was used to correct the Class II anteroposterior relationship on the Class II side and to reinforce anchorage to maintain the Class I relationship on the Class I side, in the 4 premolar extraction protocol. In the 3 premolar extraction protocol, extraoral headgear was used to reinforce anchorage to maintain the molars in Class II and Class I relationships on the respective sides. When necessary, Class II elastics were used in the 4 premolar extraction group to help obtain a Class I molar relationship on the Class II side, whereas in the 3 premolar extraction group, this procedure was used to help maintain the original molar relationship.
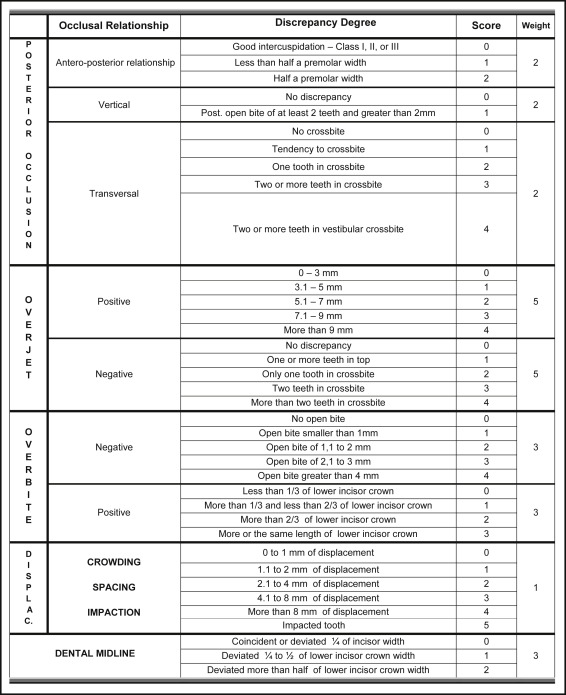
To compare the efficiency of the treatment protocol in each group, the pretreatment and posttreatment occlusal results were assessed on dental casts using the Peer Assessment Rating (PAR) occlusal index, according to the American weightings suggested by DeGuzman et al, and the time spent in the treatment of each group was calculated from the clinical charts. A form was used to calculate the PAR index on the pretreatment and posttreatment study models of each patient ( Fig ). The PAR occlusal index evaluates posterior occlusion, overjet, overbite, dental midline, and crowding.
The amounts of initial and final dental midline deviation and improvement of midline deviation correction were also evaluated with a caliper (Absolute IP67 model; Mitutoyo, Kawasaki, Japan).
Treatment efficiency (treatment efficiency index, TEI) was assessed using an index defined as the rate between the percentage of occlusal improvement (PCPAR) by the treatment time (TT) in months, expressed as TEIPAR = PCPAR/TT ( Table I ). Treatment efficiency increases when a greater percentage of occlusal improvement is associated with a shorter treatment time.
| Abbreviation | Description |
|---|---|
| IPAR | Initial PAR index |
| FPAR | Final PAR index |
| PCPAR | Percentage of improvement of the PAR index |
| TEIPAR | Treatment efficiency index of the PAR index |
| DIFPAR | Amount of improvement of the PAR index |
| TT | Treatment time |
| IAGE | Initial age |
| IMD | Initial midline deviation |
| FMD | Final midline deviation |
| CMD | Change in midline deviation |
Twenty-two pairs of dental study models were randomly selected and remeasured by the same examiner (T.B.) a month later. The random errors were calculated according to Dahlberg’s formula (Se 2 = Σd 2 /2n), where Se 2 is the error variance, and d is the difference between 2 determinations of the same variable. The systematic errors were estimated with dependent t tests at P <0.05.
Statistical analysis
Means and standard deviations for each variable were calculated to enable characterization of the groups. Normal distributions were verified by the Kolmogorov-Smirnov test. The results of this test showed that final malocclusion severity and final midline deviation were not normally distributed. Therefore, t tests were used to compare the initial malocclusion severity and age, amount of malocclusion improvement with treatment, percentage of improvement, treatment time, treatment efficiency, initial midline deviation and the change in midline deviation between the groups. Intergroup final malocclusion severity and final midline deviation were compared with Mann-Whitney tests.
All tests were performed with Statistica software (release 7; StatSoft, Tulsa, Okla), at P <0.05.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


