Introduction
The Nance appliance is widely considered to be an efficient method of anchorage reinforcement; however, much of the perceived advantage is based on clinical judgment. The aim of this study was to assess the amounts of anchorage loss and desired tooth movement associated with the Nance appliance.
Methods
The mandibular arches of 7 beagle dogs were used. The first and third premolars were extracted. Reference miniscrews were placed at the first premolar sites as stable references to measure the amounts of anchorage loss and desired tooth movement. Four beagles were fitted with custom-made Nance appliances on the fourth premolars and orthodontic bands on the second premolars (Nance group). Three beagles were fitted with orthodontic bands on the second and fourth premolars with no anchorage reinforcement (control group). The second premolars were retracted over 15 weeks in both groups. The amounts of second premolar movement (desired tooth movement) and fourth premolar movement (anchorage loss) were recorded at 5, 10, and 15 weeks. The percentages of desired tooth movement and anchorage loss to the total space closure were calculated.
Results
The mean desired tooth movement was significantly more in the Nance group than in the control group at 10 weeks ( P <0.05) but was not significantly different at 5 and 15 weeks. The mean percentages of anchorage loss to the total space closure at 15 weeks were 45.7% in the control group and 28.8% in the Nance group. The Nance group had 16.9% less anchorage loss and 16.6% more desired tooth movement than did the control group at 15 weeks ( P <0.05). Most of the anchorage loss (80%) in the Nance group occurred during the first 10 weeks.
Conclusions
The Nance appliance did not provide absolute anchorage, but there was significantly less anchorage loss with it than in the control group. The majority of anchorage loss occurred during the first 10 weeks in the Nance group.
Highlights
- •
We assessed anchorage loss and desired tooth movement associated with the Nance appliance.
- •
It provided a significant anchorage gain over the control group after 15 weeks of tooth retraction.
- •
Most anchorage loss (80%) in the Nance group occurred during the first 10 weeks.
- •
Mean anchorage losses were 28.8% in the Nance group and 45.7% in the control group.
Orthodontists are sometimes perplexed by the failure of their treatment plan to correspond with the desired results. This is often due to inadequate consideration of anchorage while forming the plan. Therefore, it is paramount to understand the biomechanical basics of anchorage before installing anchorage reinforcements. Anchorage is defined as the resistance to unwanted tooth movement. Its application in the context of orthodontics means that when a force is applied to a tooth, an equal and opposite force is distributed to the teeth opposing that force in the arch. This then leads to unwanted movement of other teeth along the arch. This undesired effect has been a perennial challenge to orthodontists. Thus, in any treatment plan, anchorage must be carefully assessed to prevent inadvertent tooth movement that may compromise the results.
Reitan found that tooth movement was slower in dense cortical bone than in medullary bone. Melsen suggested that medullary bone is more amenable to remodeling. Intraoral appliances that use the cortical bone have been used on the first molars to reinforce anchorage. These appliances enforce anchorage by maintaining a fixed intermolar width across the arch that will cause the roots of the molars to engage the buccal cortex as they move forward. The Nance appliance, a modified version of the transpalatal arch incorporating an acrylic button, has been used in patients with higher anchorage requirements. This modification is believed to overcome the anchorage loss (AL) associated with the transpalatal arch. In addition to the outer cortical bone surrounding the teeth, it is believed that the acrylic button uses the palatal cortical bone to provide additional anchorage. Until recently, much of the perceived advantage was based on clinical judgment. Two recent studies have assessed the effectiveness of the Nance appliance in providing anchorage. The results showed that the Nance appliance did not provide absolute anchorage. However, both studies lacked a control group to investigate the amount of AL without the Nance appliance. Providing a control group without anchorage reinforcement and observing AL in a clinical study is a challenge. This involves an ethical issue because AL might compromise the overall treatment. The method used by both previous studies to measure AL was not sensitive because it depended on unstable points transferred onto study casts. Furthermore, the sample of Shpack et al was not matched for age, crowding, and malocclusion, and the duration of active retraction was not controlled. Since tooth movement occurs in stages (initial, lag, postlag, and linear), AL may have varied at different stages of tooth movement during treatment. Although the sample in the other study was matched for age, malocclusion and crowding were not matched. Moreover, the AL associated with the Nance appliance was assessed only during the alignment and leveling stage of orthodontic treatment. Currently, the anchorage potential of Nance appliance has not been identified, and the stages at which AL occurs are yet to be determined. Thus, a controlled study with a specifically designed methodology to measure AL associated with the Nance appliance at different stages of tooth movement is required.
The aims of this study were to assess the amounts of AL and desired tooth movement (DTM) associated with the Nance appliance at 3 time points (5, 10, and 15 weeks) in a dog model and to compare them with a control group with no anchorage-reinforcement method.
Material and methods
Under a government license issued by the Department of Health and Children of Ireland, both the right and left mandibular sides of 7 adult male beagle dogs were used in the study (n = 14); their mean age was 16.5 (±3) months, and mean weight was 12.8 (±1.9) kg. Ethical approval was granted by the Bio-Resources Ethics Committee of Trinity College in Dublin. The study protocol was in accordance with Department of Health policies and regulations for animal care. The animals were fed a soft diet throughout the experiment.
Under general anesthesia, the mandibular first and third premolars were extracted on both sides. The first premolars were extracted to provide an edentulous ridge for miniscrew placement and the third premolars to create a space for tooth movement. The animals were left for a healing period of 3 months to allow for bone remodeling before the placement of miniscrews and to facilitate orthodontic tooth movement into an area with uniform bone structure at the third premolar extraction site. This simulated the human clinical situation because teeth are not moved immediately after extractions; rather, space closure begins after a 6- to 9-month alignment phase.
After the healing period, the animals were divided into 2 groups: 3 dogs were allocated to a control group without anchorage reinforcement (tooth anchorage) in each side of the mandible (n = 6) and 4 dogs to a Nance group in which the anchorage was reinforced with a Nance appliance in each side of the mandible (n = 8). Silicon impressions were taken for fabricating the orthodontic bands and the Nance appliances. The impressions were poured within an hour in type IV dental stone (Jade Stone; Whip Mix, Louisville, Ky) and used for the construction of the orthodontic bands and the components of the Nance appliance. Custom-made bands were cast with Vitallium 2 alloy (DENTSPLY, Hoom, The Netherlands) to fit the second and fourth premolars. The bands had tubes on the buccal aspects that allowed for the sliding of a 1-mm stainless steel wire. To ensure that the wires were passive immediately after band cementation, a wire was passed through the fourth and second premolar buccal tubes during the wax-up stage of the bands. Each band was fitted with hooks on the buccal aspect for the application of the orthodontic force. The hooks were soldered gingivally to limit tipping and encourage bodily movement because they would be closer to the center of resistance of the tooth. Finally, a reference point for recording movements was placed at the top of each band. The bands and the Nance appliances were cemented by using PANAVIA F 2.0 (Kuraray Europe, Frankfurt, Germany), a universal dual curing resin cement with high bond strength to tooth structures and metals.
Miniscrews were used as reference points for tooth movement measurements. A total of 28 self-drilling tapered miniscrews (1.3 × 7 mm) were used in the study (Absoanchor; DENTOS, Dalseo-Gu, Daegu, Korea). In both groups, each first premolar site received 2 miniscrews. One of them served as a reference miniscrew for all measurements; the other miniscrew was placed to monitor the positional stability of the reference miniscrew. A 1-mm pilot hole was drilled through the soft tissue and into the cortical bone using a 0.9-mm round bur under constant saline solution irrigation. A tunnel was made in the alveolus using a pilot drill (0.3 mm smaller than the diameter of the miniscrew) at a 30° to 60° angle to the long axis of the teeth, with the tip aiming apically. The animals were allowed to recover for 2 weeks during which antibiotics were administrated. Throughout the study, the miniscrews remained stationary because no forces were applied to them. This was confirmed by measuring the distances between them at 5-week intervals.
Tooth movement was initiated 2 weeks after miniscrew placement using 3-mm nickel-titanium coil springs (Sentalloy medium; GAC International, Bohemia, NY). A 0.01-in stainless steel wire ligature was used to tie the nickel-titanium springs to the hooks on the second and fourth premolar bands in both groups ( Fig 1 ). The force was calibrated to 150 g using a Correx tension gauge (Haag-Streit, Koeniz, Switzerland). The springs were reactivated every 5 weeks, simulating the clinical situation during orthodontic space closure. The orthodontic appliances, teeth, and gingivae were thoroughly cleaned twice a week with a toothbrush and gauzes soaked with 0.2% chlorhexidine.
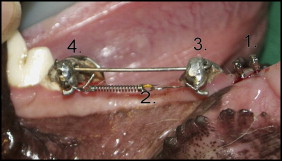
Mesial movement of the fourth premolar represented AL, whereas distal movement of the second premolar represented DTM ( Fig 2 ). A digital caliper (Absolute; Moore & Wright, Sheffield, United Kingdom) was used to measure the movements. The caliper had a resolution of 0.01 mm. Measurements were recorded at the baseline, 5 weeks (T1), 10 weeks (T2), and 15 weeks (T3). Each measurement was then repeated 3 times.

With the second and fourth premolar measurements, the amounts of DTM and AL during space closure were determined. The amount of DTM was calculated by comparing the measurements made at 5, 10, and 15 weeks with those made at baseline for the second premolars. The amount of AL was calculated in the same manner by comparing measurements made at 5, 10. and 15 weeks with those made at baseline for the fourth premolars. Both the DTM and the AL were also expressed as percentages of the total space closure at 5, 10, and 15 weeks.
The error of the measurement method was calculated according to Dahlberg’s equation : e=√∑di22n,
e = ∑ d i 2 2 n ,
in which di is the difference between duplicate measurements, and n is the number of repeated measurements. Thirty pairs of duplicate measurements for the control and Nance groups were randomly chosen. The errors of the method were found to be 0.068 mm for DTM and 0.075 mm for AL in the control group. The errors of the method were 0.069 mm for DTM and 0.029 mm for AL in the Nance group. The random errors for both groups were clinically insignificant.
Statistical analysis
The data were aggregated and averaged over repeated measures in the mandibular sides of each animal. Multilevel regression model and post hoc tests (Tukey honest significant difference) were used to allow for within-group longitudinal analysis and between-group comparisons. The parameters of interest were (1) amount of DTM, (2) amount of AL, (3) percentage of DTM, and (4) percentage of AL. Differences within groups at each time (intragroup difference) and between groups at each time (intergroup difference) were analyzed. In all cases, the significance level was set at P <0.05. The data were analyzed and graphically depicted using R software (version 2.11.1; Vienna, Austria; http://www.R-project.org ).
Results
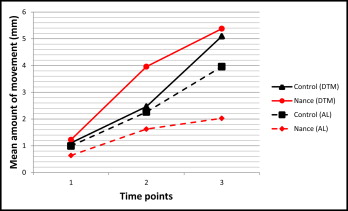
In the comparisons in the control and Nance groups for DTM, both groups showed a continuous increase in the mean amount of DTM over the 3 time points ( Fig 3 ). In the control group, the mean amounts of DTM were 1.1, 2.46, and 5.09 mm ( Table I ), and the incremental increase (mean difference) of the DTM was statistically significant only when T2 and T3 were compared ( P <0.01). In the Nance group, the mean amounts of DTM were 1.23, 3.96, and 5.38 mm ( Table I ), but the incremental increase was statistically significant when T1 was compared with T2 ( P <0.01) and T2 was compared with T3 ( P <0.05).
| Data | Time | Mean ± SD | |
|---|---|---|---|
| Control | Nance | ||
| DTM (mm) | 1 | 1.10 ± 0.90 | 1.23 ± 0.97 |
| 2 | 2.46 ± 2.41 | 3.96 ± 2.50 | |
| 3 | 5.09 ± 2.45 | 5.38 ± 2.19 | |
| AL (mm) | 1 | 0.99 ± 1.36 | 0.62 ± 0.62 |
| 2 | 2.26 ± 1.10 | 1.63 ± 1.13 | |
| 3 | 3.96 ± 1.48 | 2.03 ± 1.26 | |
| DTM (%) | 1 | 59.98 ± 28.66 | 66.24 ± 16.82 |
| 2 | 45.13 ± 23.89 | 66.90 ± 22.05 | |
| 3 | 54.51 ± 13.42 | 71.15 ± 15.73 | |
| AL (%) | 1 | 40.02 ± 28.66 | 33.75 ± 16.82 |
| 2 | 54.85 ± 23.89 | 33.04 ± 22.05 | |
| 3 | 45.68 ± 13.42 | 28.75 ± 15.73 | |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


