Introduction
Orthodontic appliances hinder mechanical plaque control. In this study, we evaluated the effect of self-performed supragingival plaque removal with ultrasonic, electric, and manual toothbrushes on subgingival plaque composition in orthodontically banded molars.
Methods
Twenty-one patients wearing fixed orthodontic appliances were assigned to this single-blind crossover study. Samples of subgingival plaque were collected from banded molars, before and after each toothbrush usage period, for quantification of 22 bacterial species by the checkerboard DNA-DNA hybridization method. For each crossover, patients used a toothbrush for 30 days, followed by a washout period of 14 days.
Results
The prevalence of Tannerella forsythia decreased significantly after a month of electric brush usage. In the manual brush group, the prevalences of Selenomonas noxia , Streptococcus sanguinis, and Prevotella melaninogenica also decreased significantly. However, there were no significant differences in the prevalences and levels of bacteria after usage of the ultrasonic brush. Intergroup comparisons showed no statistical differences among the 3 brushes for the microbiologic parameters.
Conclusions
All 3 brushes generally reduced bacterial prevalences, and, although electric and manual toothbrushes showed some isolated significant variations, we found no superiority with any toothbrush type when used three times daily for 2 minutes on microbiologic parameters in orthodontically banded molars.
The contribution of dental plaque control to prevent caries and periodontal diseases is well established. Experimental gingivitis studies have clearly shown that gingival inflammation is treated by the removal of accumulated dental plaque. Plaque removal by manual toothbrushing is the most common method of oral hygiene in the world. Because so much effort is directed at controlling organisms by this means, it is surprising that few studies have examined the changes in plaque composition from this procedure. The few published studies have used culture media, DNA probes, or, more recently, checkerboard DNA-DNA hybridization.
Patients undergoing orthodontic therapy face greater difficulties maintaining good oral hygiene than other patients. Orthodontic appliances with bands, brackets, and arches are barriers for brush bristles and dental floss, leading to greater accumulations of plaque and impairment of gingival health. Orthodontic treatment with fixed appliances is highly associated with gingival inflammation and bleeding, gingival enlargement, and increased probing pocket depths.
Microbiologic subgingival changes have also been associated with the placement of fixed orthodontic appliances. Studies have shown decreases in gram-positive cocci, which are associated with periodontal health, and statistically significant increases in suspected periodontal pathogens such as spirochetes, motile rods, and other gram-negative organisms.
Data examining the effects of various toothbrushes on subgingival plaque composition of patients with orthodontic appliances are sparse. No study has reported the efficacy of an ultrasonic toothbrush used by orthodontic patients on subgingival plaque. Thus, the purpose of this investigation was to determine the effect of self-performed supragingival plaque removal with ultrasonic, electric, and manual toothbrushing on subgingival plaque composition in these patients. The clinical changes in these subjects were described elsewhere.
Material and methods
Twenty-one adolescent patients (11 boys, 10 girls; age range, 12-18 years; average, 15.2 ± 1.7 years) undergoing orthodontic treatment at the School of Dentistry at São Paulo State University, Araraquara, Brazil, were consecutively selected for this study.
Each had at least 20 teeth and had been in orthodontic treatment with fixed appliances for a minimum of a year. All were nonsmokers with no obvious periodontal disease or attachment loss. They had taken no medications in the last 3 months and had no systemic or local disease affecting the periodontium. According to the protocol of the orthodontic clinic, all patients received plaque control and instructions in oral hygiene before treatment, and periodontal conditions were regularly evaluated during treatment.
This study was a single-blind crossover clinical trial. It was approved by the Ethics and Research Committee of the School of Dentistry of São Paulo State University.
The ultrasonic brush tested was the Ultrasonex Ultima Toothbrush (Sonex International, Brewster, NY), which has a removable center head and operates at a frequency of 1.6 MHz. Comparisons were made with an electric brush (Braun Oral B 3D Plaque Remover, Braun GmbH, Kronberg, Germany) and a manual brush (Oral B Model 30, Gillete do Brasil, Manaus, Brazil).
The participants were randomly divided into 3 sequences of brush use: (1) ultrasonic, electric, and manual; (2) manual, ultrasonic, and electric; and (3) electric, manual, and ultrasonic.
The sequence distribution of the patients was done to eliminate the influence of the Hawthorne effect on the results, after each type of brush was used by a group of patients in the 3 periods of the study.
The subjects used each assigned brush for 30 days followed by14 days when they returned to the toothbrush and dental floss usage according to the instructions from their orthodontist before the study. The patients were evaluated at the end of morning or afternoon periods with 3 to 5 hours of plaque accumulation both at baseline and after every 30-day period. During baseline visits, the subjects were instructed in oral-hygiene techniques. For those receiving a manual brush, the Bass technique was demonstrated; those receiving the electric and ultrasonic versions were given audiovisual presentations on the correct use according to the manufacturers followed by a session for personal instruction and answering questions. The subjects were asked to use their assigned toothbrush 3 times daily for 2 minutes with a designated toothpaste (Sorriso, Colgate-Palmolive Indústria e Comércio Ltda, São Bernardo do Campo, São Paulo, Brazil) and to avoid other oral health products or techniques.
Clinical measurements were presented previously. Briefly, plaque and gingival inflammation were assessed on all teeth except the second and third molars by using the plaque index of Silness and Löe and the gingival index of Löe and Silness, respectively. The orthodontic modification of the plaque index was used on the buccal surfaces of the teeth because of the brackets. Probing depth was measured at 6 sites per tooth. All measurements were done by a calibrated examiner (M.R.C.).
Clinical and microbiologic monitoring was done at baseline and 4 weeks after the use of each brush.
The presence and levels of 22 species were determined by a modification of the checkerboard DNA-DNA hybridization method described by Socransky et al.
Individual subgingival plaque samples were obtained from the 4 first molars (banded teeth) in each subject at baseline and after the period of use of each brush. After removal of supragingival plaque, subgingival plaque samples were taken from the mesiobuccal line angle area of each tooth by using sterile Gracey curettes. Each sample was placed in a tube containing 0.15 mL TE (10 mmol/L Tris-hydrochloric acid, 1 mmol/L EDTA, pH 7.6). Then, 0.10 mL of 0.5 M sodium hydroxide was added to each sample, and the tubes were frozen for future analysis. After this, the cells were lysed, and denatured DNA was fixed in individual lanes on a nylon membrane by using the checkerboard slot blot device. Twenty-two digoxigenin-labeled whole genomic DNA probes were hybridized at 90°C to the lanes of the plaque samples. Bound probes were detected by using phosphatase-conjugated antibody to digoxigenin and chemiluminescence. Signals were evaluated visually by comparison with the standards at 10 5 and 10 6 bacterial cells for the test species on the same membrane. They were recorded as 0, not detected; 1, <10 5 cells; 2, about 10 5 cells; 3, 10 5 to 10 6 cells; 4, about 10 6 cells; and 5, >10 6 cells. The sensitivity of this assay was adjusted to permit the detection of 10 4 cells of a species by adjusting the concentration of each DNA probe. This procedure was carried out to provide the same sensitivity of detection for each species.
Failure to detect a signal was recorded as zero, although counts in the 1 to 10,000 range could conceivably have been present. A total of 504 plaque samples were evaluated.
Statistical analysis
The mean frequency of levels (0-5) of each species was computed for each subject and then averaged across subjects in the 3 toothbrush groups (manual, electric, or ultrasonic). In addition, the percentages of sites colonized by each species (prevalence) were also computed for each subject and averaged across subjects in the 3 groups. The significance of differences in mean percentages of sites colonized by subgingival species among the 3 groups was determined by using the Kruskal-Wallis test. Changes in plaque composition over time (baseline to 1 month) were evaluated by using the Wilcoxon test. Statistical significance was set at P = 0.05.
Results
All 21 patients completed the study with no adverse effects reported by any of them or noted by the examiner (M.R.C.). Clinical results showed no significant differences among brush groups. However, the ultrasonic toothbrush showed significant improvement in the reduction of visible plaque on the buccal surfaces, with a tendency to remove more plaque around the brackets.
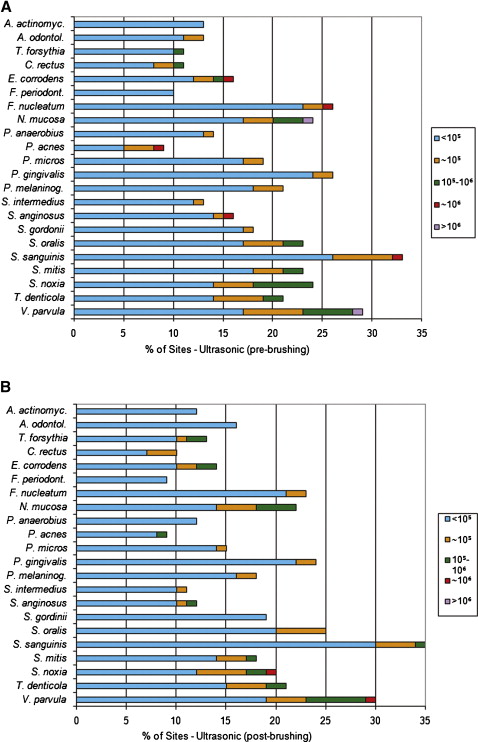
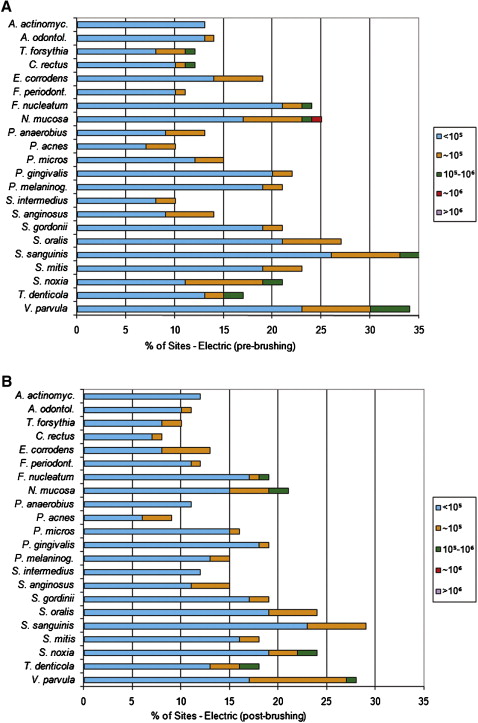
Figures 1, 2, and 3 summarize the prevalence of the colonized sites and the levels of the 22 subgingival species in the 3 brush groups. The most frequently detected species in all samples and subjects included Fusobacterium nucleatum , Neisseria mucosa , Streptococcus oralis , S sanguinis , and Veillonella parvula . The least prevalent species were Actinobacillus actinomycetemcomitans , F periodonticum , Campylobacter rectus , Propionybacterium acnes , and S intermedius . At baseline, there were no statistical differences among the 3 brush groups for the 22 species evaluated ( P >0.05, Kruskal-Wallis test).