Introduction
Infrabony defects in the alveolus pose a substantial treatment complication for restorative dentists. The properties of regenerate bone produced by dentoalveolar distraction, with and without a latency period, remain largely unknown.
Methods
Six male foxhound dogs between 1 and 2 years of age underwent osteotomies around the mandibular second premolar to create a dentoalveolar segment that was distracted (1 mm/day for 10 days) through a large periodontal defect created in the third premolar area. A split-mouth design was used, with 1 randomly selected side starting distraction immediately, and the other side starting distraction after a 5-day latency period. The nonlatency and latency sides had 7 and 6 weeks of consolidation, respectively. Microcomputed tomography scans (taken at 15 and 60 μm) were used to evaluate bone quality and quantity of the regenerate bone, as well as the maturational differences in the regenerate.
Results
The transport segments were distracted 7 to 8 mm over 10 days. The majority (>75%) of the specimens showed complete or almost complete vertical and buccolingual bone fill. Except for trabecular separation, there were no significant differences between the latency and nonlatency sides in the quantity or quality of bone produced. Although relative bone volume tended to increase between the mesial and distal aspects of the regenerate, there were no significant differences in material properties in the regenerate. The control bone was denser and greater in quantity than the regenerate bone.
Conclusions
Except for slight differences in maturation, latency had little or no effect on the regenerate bone produced. Dentoalveolar distraction immediately after alveolar bone surgery appears to produce bone of adequate quantity and quality for dental implant restorations.
The most common treatment modalities for restoring single-tooth edentulous sites are implant-supported crowns and conventional fixed partial dentures. Successful placement of dental implants requires an adequate quantity and quality of bone, not only vertically, but also mesiodistally (1.5 mm) and buccolingually (1 mm). Successful fixed partial dentures require a crown:root ratio greater than 1:1 and no mobility of the abutment teeth. Unfortunately, neither implants nor fixed partial dentures address the problems associated with severe alveolar defects that can be associated with edentulous spaces secondary to long-term resorption related to traumatic extractions. Such cases require additional procedures such as bone grafting and bone regeneration to meet the patient’s functional and esthetic restorative demands. Dentoalveolar distraction might provide a technique for better repair of bony alveolar defects.
Recently, dentoalveolar distraction has been used to rapidly move canines through extraction sites in humans. The technique involves extraction of the maxillary first premolars, corticotomies around the root of the canine, and removal of the buccal plate and the interseptal bone distal to the canine. The dentoalveolar segment is then fully mobilized and rapidly distracted into the extraction site (ie, dentoalveolar bone transport). Osteotomies separate the dentoalveolar segment from the mesial and apical bone; this is thought to promote angiogenesis and bone healing from an increased vascular supply to the dentoalveolar segment. The surrounding bone and the potential for increased vascularity differentiate dentoalveolar distraction from traditional distraction osteogenesis. The biologic properties of regenerate bone after dentoalveolar distraction have not been well described; little is known about bone regenerate quality and quantity produced by dentoalveolar distraction.
The success of distraction procedures is thought to be influenced by the amount of trauma during surgery, the rate and rhythm of distraction, the stability of the segments, and a latency period. Yasui et al showed that immediate distraction after surgery led to callus retardation in long bones, which they attributed to the disruption of the vascularity. However, the latency criteria currently used are based on our understanding of traditional distraction of long bones; different latency periods might be required for dentoalveolar distraction. Craniofacial distraction in various animal models suggests that a latency period might be unnecessary. The effects of latency on the regenerate bone produced in craniofacial distraction, especially dentoalveolar distraction, have not been verified experimentally.
On that basis, the purpose of this study was to evaluate the dimensional quality and quantity of regenerate bone produced with and without a latency period. Because of the unique differences between dentoalveolar distraction and traditional distraction osteogenesis, this study was designed to compare the maturation of bone in the regenerate. The regenerate bone was compared with adjacent control bone to determine whether the regenerate bone could be considered suitable for dental implant placement.
Material and methods
Six male foxhound dogs between 1 and 2 years of age were used as the experimental model. Their weights ranged from 55 to 65 lbs. The handling of the dogs, the methods used to fabricate the distraction devices, the bonding procedures used, and the surgical procedures were fully described in the companion article by Spencer et al.
Die stone models from alginate impressions were used to fabricate the distraction devices, consisting of hyrax expansion screws (Dentaurum, Ispringen, Germany) soldered onto stainless steel bands made to fit the mandibular canines and second premolars.
A horizontal crestal incision was made from the first molar to the canine, and a full-thickness mucoperiosteal flap was reflected by using a periodontal elevator ( Fig 1 , A ). Vertical osteotomy cuts were made 1 mm mesial and distal to the roots of the second premolar; a horizontal cut was made 1 mm apical to the roots of the second premolar, just above the inferior alveolar neurovascular bundle. A large rectangular segment of bone in the area of the third molars was surgically removed to create a severe periodontal defect ( Fig 1 , B ). The dentoalveolar segment, which included the fourth premolar, was distracted into the defect. The dentoalveolar transport segment was completely mobile except for the lingual mucosal attachment, which was not disrupted from the alveolar bone to maintain blood supply.
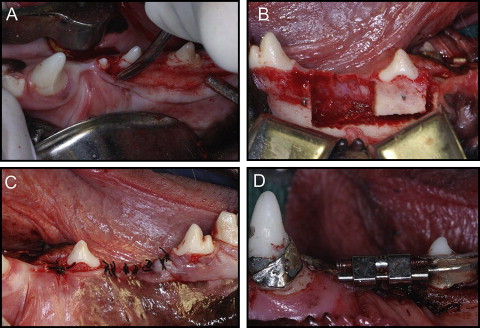
After wound closure ( Fig 1 , C ), the mandibular canines and the second premolars were etched with 37% phosphoric acid gel for 30 seconds. All-Bond 2, primer A and B (Bisco, Richmond, British Columbia, Canada), were mixed and applied to each tooth; after 10 seconds, All-Bond 2 adhesive resin was applied and cured for an additional 10 seconds. The bands were filled with the 3M Filtek Supreme restorative composite resin (3M ESPE, St Paul, Minn) and seated onto the prepared teeth. Once the distractors were seated ( Fig 1 , D ), the composite was light-cured for 40 seconds per tooth. The maxillary and mandibular canines and premolars were equilibrated to prevent traumatic occlusion. Pulpotomies were performed on 2 dogs because of occlusal interferences.
One randomly selected side of the mandible was distracted after a 5-day latency period; the other side was distracted immediately. Based on the study of Hasse et al, the segments were distracted at a rate of 1 mm per day (4 turns of the distractor at 1 time) for 10 days.
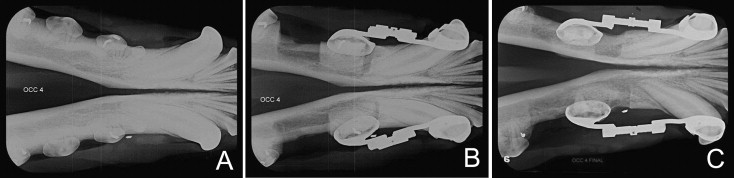
To measure the movements of the distracted segments, intraoral caliper measurements were made between notches drilled into the mesial aspect of the canine and the distal aspect of the second premolar ( Fig 1 , D ). Occlusal radiographs were taken to monitor distraction and bone healing. The measurements and occlusal radiographs were taken before surgery, immediately after surgery, and every 3 days until the distraction protocol had been completed ( Fig 2 ).
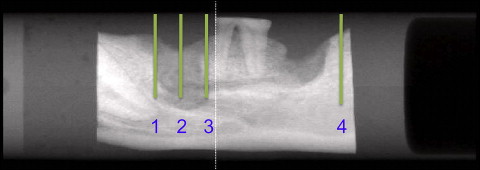
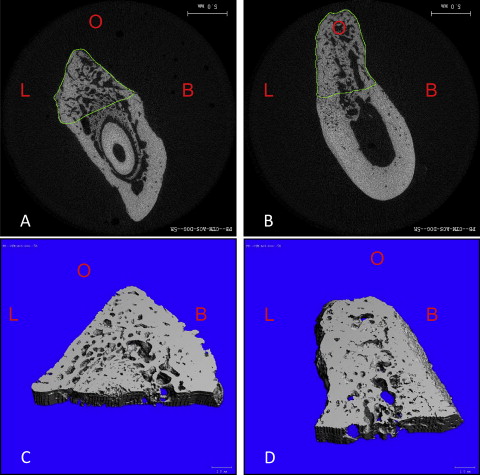
Specimens were placed in 27-mm long scanning tubes and loaded into the Scanco Micro-CT 35 scanner (Scanco Medical, Bassersdorf, Switzerland). A preview radiograph was used for defining the volumes of interest ( Fig 3 ). The entire specimen was then scanned at 60 μm to obtain an overall digital 3-dimensional reconstruction and qualitative evaluation of bone loss in the regenerate areas. Four additional scans were taken at a higher resolution (15 μm) for quantification of bone structure. The regenerate bone was divided into 3 volumes (mesial, middle, and distal) that were compared with the control volume from a comparable region. Each volume included 100 slices; each slice was traced ( Fig 4 ), and the regenerate and control volumes were segmented by the examiner (C.M.) with the Micro-CT software (version 6.0, Scanco). Bone trabecular morphometry software (Scanco) was used to estimate bone density, bone volume fraction, trabecular number, trabecular thickness, and the space between trabeculae referred to as trabecular separation.
Statistical analysis
Statistical analyses were performed by using SPSS software (version 15; SPSS, Chicago, Ill). Nonparametric Friedman tests and Wilcoxon signed rank tests were used to analyze differences between regenerate bone and control alveolar bone. Wilcoxon signed rank tests were used to examine differences between the latency and nonlatency sides.
Results
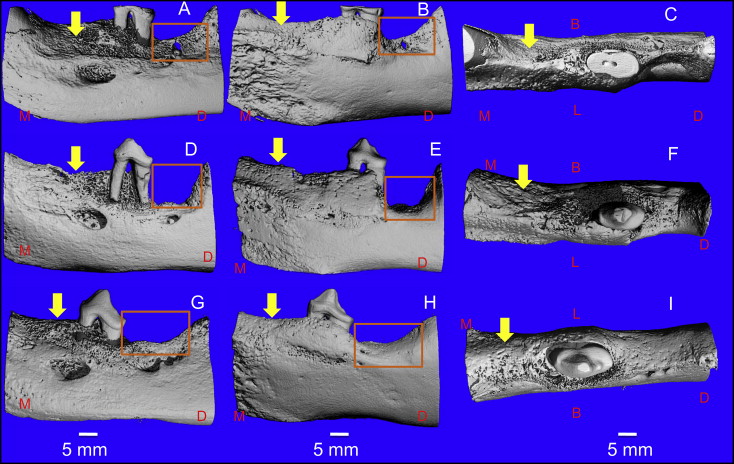
The latency and nonlatency regenerate bone exhibited similar morphologies. Overall, the regenerate displayed a less mature mineralization pattern than did the control alveolar bone; the regenerate was composed primarily of trabecular bone, with only trace amounts of cortical bone. Two of the 12 specimens had complete vertical bone fill in the regenerate region, 7 showed slight (1-2 mm) vertical defects, and 3 showed moderate (2-4 mm) vertical defects ( Fig 5 ). From the occlusal aspect, 11 specimens exhibited complete bone regeneration in a buccolingual direction, and 1 specimen showed a slight resorptive pattern. Whereas all specimens had moderate to severe (>4 mm) loss of bone on the buccal surface of the transport segment overlying the tooth, the buccal surface of the regenerate did show adequate bony width. The lingual surface of the regenerate consistently showed greater mineralization than did the buccal surface.
New bone had partially filled the remaining defect distal to the distracted dentoalveolar segment, although the amount of fill was substantially less than that in the regenerate area. Five specimens showed 10% to 30% new bone fill, and 7 had 40% to 60% fill.
In comparison with the regenerate bone, the control bone was denser and greater in quantity, as well as greater in trabecular thickness with fewer trabeculae ( Tables I and II ). Trabecular separation was similar for the regenerate and the control bones. The control bone was statistically different from the nonlatency regenerate for bone volume fraction, density (nonlatency side only), trabecular number, and trabecular thickness.
| Variable | Unit | Distal regenerate | Middle regenerate | Mesial regenerate | Control bone | All 4 sections | Regenerate sections | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | P | P | ||
| Bone volume fraction | % | 0.47 | 0.06 | 0.51 | 0.12 | 0.52 | 0.12 | 0.67 | 0.04 | 0.010 ∗ | 0.607 |
| Bone density | mgHA/ccm | 792 | 38 | 763 | 70 | 807 | 70 | 893 | 46 | 0.009 ∗ | 0.607 |
| Trabecular separation | mm | 0.20 | 0.06 | 0.16 | 0.04 | 0.19 | 0.03 | 0.21 | 0.04 | 0.060 | 0.115 |
| Trabecular sumber | mm | 2.88 | 0.72 | 3.11 | 0.85 | 2.59 | 0.70 | 1.63 | 0.48 | 0.004 ∗ | 0.115 |
| Trabecular thickness | mm | 0.17 | 0.05 | 0.19 | 0.13 | 0.23 | 0.11 | 0.45 | 0.15 | 0.007 ∗ | 0.311 |
| Variable | Unit | Distal regenerate | Middle regenerate | Mesial regenerate | Control bone | All 4 sections | Regenerate sections | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | P | P | ||
| Bone volume fraction | % | 0.45 | 0.06 | 0.51 | 0.15 | 0.53 | 0.13 | 0.67 | 0.02 | 0.024 ∗ | 0.607 |
| Bone density | mgHA/ccm | 815 | 31 | 801 | 76 | 792 | 68 | 893 | 48 | 0.187 | 1.000 |
| Trabecular separation | mm | 0.24 | 0.04 | 0.20 | 0.03 | 0.18 | 0.04 | 0.21 | 0.04 | 0.086 | 0.069 |
| Trabecular number | mm | 2.38 | 0.34 | 2.42 | 0.63 | 2.75 | 0.96 | 1.63 | 0.38 | 0.024 ∗ | 0.311 |
| Trabecular thickness | mm | 0.19 | 0.04 | 0.26 | 0.14 | 0.23 | 0.14 | 0.45 | 0.11 | 0.012 ∗ | 0.846 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


