Introduction
Our objective was to compare the effects of 3 light-curing units (LCUs) (quartz-tungsten-halogen [QTH], light-emitting diode [LED], and plasma-arc curing [PAC]) on the microleakage patterns of a polyacid-modified composite (PAMC) for band cementation between the cement-enamel and the cement-band interfaces from the buccal, lingual, occlusal, and gingival margins.
Methods
Sixty freshly extracted third molars were randomly divided into 3 groups of 20 teeth each. Microetched molar bands were cemented in all groups with the PAMC (Ultra Band-Lok, Reliance Orthodontic Products, Itasca, Ill) and cured for 30 seconds with the QTH (Hilux 350, Express Dental Products, Toronto, Ontario, Canada), for 20 seconds with the LED (Elipar Freelight 2, 3M Espe, Seefeld, Germany), or for 6 seconds with the PAC (Power-Pac, American Medical Technologies, Hannover, Germany). A dye penetration method was used for microleakage evaluation. Microleakage was determined with a stereomicroscope for the cement-band and cement-enamel interfaces from the buccal and lingual sides at the occlusal and gingival margins. Statistical analyses were performed with the Kruskal-Wallis and Mann-Whitney U tests. The level of significance was set at P <0.05.
Results
The gingival sides in the LED and PAC groups had higher microleakage scores compared with those observed on the occlusal sides at both the cement-band and cement-enamel interfaces. The buccal sides had similar microleakage values compared with those on the lingual sides for the cement-enamel and cement-band interfaces in all LCU types. Statistical comparisons showed that there were statistically significant differences among the investigated LCUs at the cement-enamel interface ( P <0.05). Post hoc comparisons showed statistically significant microleakage differences between the PAC (median, 0.950 mm), the QTH (median, 0.383 mm) ( P <0.01), and the PAC and the LED (median, 0.558 mm) ( P <0.05) LCUs at the cement-enamel interfaces.
Conclusions
The high-intensity curing device PAC is associated with more microleakage than the LED and QTH at the cement-enamel interface.
Until recently, the most popular light-curing unit (LCU) in dentistry was the quartz-tungsten-halogen (QTH). Then, manufacturers brought out plasma-arc curing (PAC) lights, argon lasers, and solid-state light-emitting diodes (LEDs) as alternatives to QTH curing units. These high-intensity curing units have been recommended universally because they enhance monomer conversion and decrease curing time.
Various visible light-cured orthodontic adhesives are commercially available. High early bond strength, minimal oxygen inhibition, and longer working time for optimal bracket or band placement are the advantages of visible light-cured orthodontic adhesives. Their major disadvantage is that they shrink during polymerization, causing shrinkage strain, marginal gaps, and eventually marginal leakage (microleakage) at the tooth-adhesive interface.
Microgap formation between the adhesive material and the enamel surface contributes to microleakage, permitting the passage of bacteria and oral fluids, which can cause white spot lesions or demineralization under the attachment surface area. In restorative dentistry, the clinical symptoms associated with microleakage are breakdown and discoloration of margins, secondary caries, and increased postoperative sensitivity and pulp pathology. Orthodontic applications usually involve thin layers of adhesives and lack areas of bulk material that would seem to favor chemical cure systems. Orthodontic bands, however, are susceptible to areas of variable cement thickness and have a physically greater barrier to irradiation than brackets. From the orthodontic point of view, one can assume that demineralization areas at and under the cement or enamel can occur because of microleakage.
The latest materials developed for cementing orthodontic bands are polyacid-modified composite (PAMC) resins. Other dental materials have been used as orthodontic cements over the years, but interest has now focused on resin-based materials. Williams et al investigated the effectiveness of a conventional glass poly(alkenoate) cement and PAMC to retain orthodontic bands and found no significant differences in the in-vitro median force to deband or the in-vivo band failure rates between investigated materials.
Uysal et al compared the microleakage patterns of conventional glass ionomer cement, resin-modified glass ionomer cement, and PAMC for band cementation and found that teeth banded with resin-modified glass ionomer cement and PAMC had similar microleakage scores; both had statistically less leakage than did the conventional glass ionomer cement.
In the orthodontic literature, the effects of different LCUs (QTH, LED, and PAC) on microleakage under lingual retainer adhesives and orthodontic brackets were investigated, but, so far to our knowledge, no study has compared the effect of these 3 LCUs on microleakage under orthodontic bands. Thus, the objective of this study was to compare the effects of 3 LCUs (QTH, LED, and PAC) on the microleakage patterns of a PAMC for band cementation at the cement-enamel and the cement-band interfaces from the buccal and lingual sides at the occlusal and gingival margins.
In this study, the null hypothesis assumed that the type of LCU (QTH, LED, or PAC) would not affect the amount of microleakage observed under the orthodontic bands.
Material and methods
Sixty caries-free extracted mandibular third molars were collected and stored in distilled water in a refrigerator after decontamination in 0.5% chloramine. The teeth were randomly divided into 3 groups of 20 teeth each.
The teeth were then cleaned with pumice, rinsed in distilled water, and dried thoroughly in a stream of air. Because there are no bands for third molars, mandibular permanent first molar bands with microetched fitting surfaces (G&H Wire, Greenwood, Ind) were used. A band was selected and adapted optimally to the crown of each tooth. The selected bands were cemented to the teeth with Ultra Band-Lok (Reliance Orthodontic Products, Itasca, Ill) light-cure band adhesive paste. After band placement, excess cement was removed with dry cotton rolls and light-cured with the following procedures according to manufacturers’ instructions.
-
Group 1: the 20 teeth were polymerized for 30 seconds with a QTH LCU (Hilux 350, Express Dental Products, Toronto, Canada) with a 10-mm diameter light tip.
-
Group 2: the 20 teeth were cured with an LED LCU (Elipar Freelight 2, 3M Espe, Seefeld, Germany) for 20 seconds.
-
Group 3: the 20 teeth were cured with a PAC LCU (Power Pac, American Medical Technologies, Hannover, Germany) for 6 seconds.
In all groups, the LCUs were applied to the bands from the occlusal direction according to manufacturers’ recommendations. To standardize the specimen preparations, band selection and cementation were done by 1 operator (S.I.R.). All specimens were then placed in distilled water for 24 hours before measuring the microleakage.
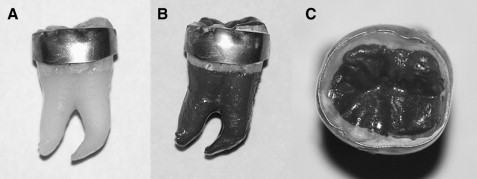
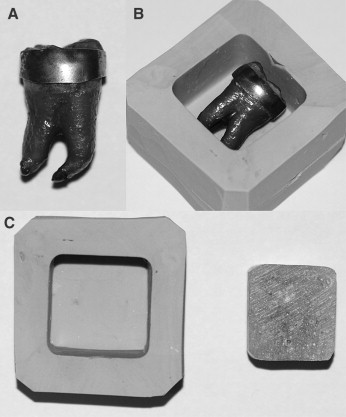
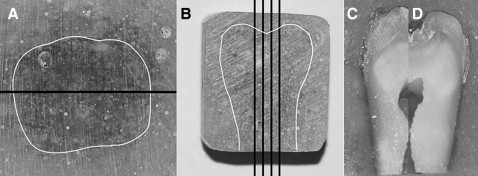
For the microleakage evaluation and before dye penetration, the tooth apices were sealed with sticky wax. After that, the teeth were rinsed in tap water and air dried, and nail varnish was applied to the entire surface of the tooth except for the area approximately 1 mm from the bands ( Fig 1 ). To minimize dehydration of the specimens, the teeth were replaced in water as soon as the nail polish dried. The teeth were immersed in 0.5% solution of basic fuchsine for 24 hours at room temperature. After removal from the solution, the teeth were rinsed in tap water, and the superficial dye was removed with a brush; the teeth were dried and embedded in self-curing acrylic up to the occlusal surface of the band ( Fig 2 ). First, all teeth were separated into 2 parts in the mesiodistal direction ( Fig 3 ). Four parallel longitudinal sections from the middle of the molars were made at the occlusal and gingival margins at buccal and lingual sides with a low-speed diamond saw (Isomet, Buehler, Lake Bluff, Ill) in the buccolingual direction according to the methods of Arikan et al and Arhun et al for the evaluation of microleakage under orthodontic brackets.
The specimens were evaluated first under a stereomicroscope (20 times magnification) (SZ 40, Olympus, Tokyo, Japan) for dye penetration along the cement-band interface. Then the band materials were gently removed from the cement, and the dye penetration at the cement-enamel interface was also evaluated under a stereomicroscope. Two assessors (M.U. and H.E) blinded to the LCU type evaluated the specimens.
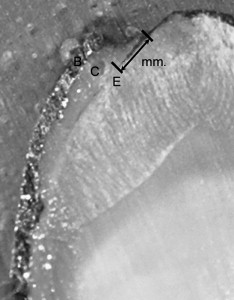
To determine the amount of microleakage, an electronic digital caliper was used for measuring the distance that the dye penetrated along the cement-band and cement-enamel interfaces on the longitudinal sections; the data were recorded to the nearest 0.5 mm ( Fig 4 ) (range, 0.5-5 mm). Each section was scored from the occlusal, gingival, buccal, and lingual margins of the bands at the cement-band and cement-enamel interfaces.
Statistical analysis
For the cement-band and cement-enamel interfaces, the microleakage score was obtained by calculating the mean of the 4 parallel longitudinal sections of the occlusal, gingival, buccal, and lingual microleakage scores.
The Shapiro-Wilks normality test and the Levene variance homogeneity test were applied to the microleakage data. The data showed nonnormal distribution, and there was no homogeneity of variances among the groups. Thus, the microleakage values between test groups were statistically evaluated by using nonparametric tests (Kruskal-Wallis and Mann-Whitney U tests). Intraexaminer and interexaminer method errors were evaluated with the kappa test. The level of significance was set at P <0.05.
Results
The intraexaminer and interexaminer kappa scores for microleakage at the buccal and lingual sides were high, with all values greater than 0.75.
Comparisons of the microleakage scores of PAMC under the orthodontic bands between the occlusal and gingival margins for the cement-band and cement-enamel interfaces at the buccal and lingual sides are shown in Table I . The gingival sides in all PAC and LED groups had higher microleakage scores compared with those observed on the occlusal sides at both cement-band and cement-enamel interfaces. At the buccal sides, except for microleakage at the cement-band interface cured by the QTH light, statistically significant differences were found between the occlusal and gingival margins’ microleakage scores. The highest statistically significant occlusal-gingival leakage differences were observed with the LED curing unit at the cement-enamel interfaces (occlusal microleakage median, 0.250 mm; gingival microleakage median, 0.875 mm) ( P <0.01). No statistically significant occlusal-gingival microleakage differences were determined at the lingual side between the cement-band and cement-enamel interfaces for any LCU type ( P >0.05).
| Side | Interface | Curing unit | n | Margin | Statistical comparison P value | |
|---|---|---|---|---|---|---|
| Occlusal | Gingival | |||||
| Median | ||||||
| Buccal | Cement-enamel | PAC | 20 | 0.625 | 0.750 | ∗ |
| LED | 20 | 0.250 | 0.875 | † | ||
| QTH | 20 | 0.250 | 0.500 | ∗ | ||
| Cement-band | PAC | 20 | 0.375 | 0.500 | ∗ | |
| LED | 20 | 0.250 | 0.500 | ∗ | ||
| QTH | 20 | 0.375 | 0.375 | NS | ||
| Lingual | Cement-enamel | PAC | 20 | 0.375 | 0.625 | NS |
| LED | 20 | 0.500 | 0.625 | NS | ||
| QTH | 20 | 0.500 | 0.625 | NS | ||
| Cement-band | PAC | 20 | 0.500 | 0.625 | NS | |
| LED | 20 | 0.375 | 0.500 | NS | ||
| QTH | 20 | 0.375 | 0.250 | NS | ||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


