Introduction
Low-level laser therapy (LLLT) has many biostimulative effects such as acceleration of mesiodistal orthodontic tooth movement. However, its effects on the extent and short-term stability of rotational tooth movement have not been researched. The purpose of this study was to investigate the effect of low-level laser irradiation during rotational tooth movement on the rate of movement and the amount of relapse in dogs.
Methods
In this interventional study, fixed orthodontic appliances were used to rotate both mandibular lateral incisors in 8 dogs. Sixteen teeth were divided into 2 groups: the experimental group with LLLT during orthodontic force application, and a control group with orthodontic couple force application only. In the first group, the gallium-aluminum-arsenide diode laser (810 nm, 200 mw, 10 seconds, 2 J/session, 32 J/cm 2 /point) was emitted on 2 points at the buccal side of the roots on days 0, 1, 2, 3, 4, 7, 14, 21, and 28 during 4 weeks of movement, and the amount of relapse was then observed for 3 months. The extent of rotational movement was measured on dental casts, and the statistical analysis was carried out with t tests.
Results
There was no significant difference between the LLLT group and the control group on the amount of rotational tooth movement ( P = 0.66). The mean percentages of relapse after 1 week, 1 month, and 3 months were 33.02%, 53.44%, and 60.64% in the LLLT group and 54.22%, 68.74%, and 73.92% in the control group, respectively. This demonstrates significant differences between these groups at all studied times ( P ≤0.05). This difference was greatest in the first week and then decreased until the end of the third month. The greatest percentage of relapse in both groups was registered in the first week after tooth movement.
Conclusions
The total energy dose of the laser used in this study could not accelerate rotational tooth movement, but it did effectively reduce the relapse tendency in teeth rotated by orthodontic movements.
Highlights
- •
Low-level laser therapy (LLLT) during orthodontic movement was evaluated in dogs.
- •
LLLT has no effect on the rate of rotational movement.
- •
LLLT can significantly increase the short-term stability of rotational movement.
- •
The effect of LLLT on the stability of rotational movement is reduced by time.
- •
The highest percentage of relapse is in the first week after orthodontic rotational movement.
Orthodontic treatment is performed to improve a patient’s smile, facial appearance, and quality of life. The tendency of teeth to return to their former positions, called relapse, is an inevitable reality in orthodontic treatment that may lead to the patient’s frustration and consequent problems for the orthodontist. Long-term usage of retainers is one of the most widespread methods to prevent relapse. However, retainers cannot stop relapse completely, particularly after rotational movements of teeth. Currently, a supracrestal fiberotomy is one of the most effective methods to decrease the rate of relapse after rotational tooth movements. This procedure stimulates the remodeling of periodontal fibers in their new positions, but it can be accompanied by several complications as well.
Recently, the effect of low-level laser therapy (LLLT) on remodeling of both soft and hard tissues surrounding the teeth has been confirmed. Tooth movement mechanisms, both during and after orthodontic treatment, are based on selective stimulation of bone remodeling. It has been shown that LLLT affects both the activity of the osteoblasts and osteoclasts and the release of the inflammatory mediators in the periodontal tissues, all of which are key elements in orthodontic tooth movement. Therefore, it can be speculated that LLLT can have a positive role in the overall rate of tooth movement.
Several studies have explored the effects of LLLT on mesiodistal tooth movements. Other dental movements such as the rotational movements that might be requisite in orthodontic treatments have not been taken into account. Moreover, because of various bone remodeling patterns in different dental movements, the results of the previously mentioned studies cannot be generalized to all orthodontic movements without further investigations.
LLLT may reduce the relapse of orthodontic treatments by increasing tissue remodeling as well as bone density. This hypothesis suggests a noninvasive physiologic method to prevent or reduce relapse. Nevertheless, only a few studies have investigated the effects of LLLT on the relapse of dental movements after orthodontic treatments. An important reason for relapse after orthodontic rotational movement is considered to be the gingival and transseptal fibers of the periodontium that are stretched and warped. LLLT can biostimulate collagen synthesis and speed up bone and dental fiber remodeling during tooth movement. This may, in turn, increase the stability of these rotated teeth and decrease the rate of relapse. Therefore, this study was designed to evaluate the effectiveness of LLLT during orthodontic rotational movement and its stability after treatment.
Material and methods
This study was conducted based on the principles of animal rights defined by the Vice-Chancellery of Shiraz University of Medical Sciences, Shiraz, Iran. The sample size was based on the combination of our limitations (ethics and time) and the degree of relapse reported by Kim et al. With α = 0.05 and a power of 80%, and because the teeth on the right and left sides of each dog acted as the control and LLLT groups, respectively, 8 dogs were needed for the study.
The study was performed with 8 healthy male beagles between 12 and 18 months of age and weighing 18 to 24 kg. Intraoral examinations confirmed that all permanent teeth were erupted, with no caries or mobility. There was neither localized nor generalized gingivitis, and the absence of ankylosis was ensured by percussion tests.
Sixteen mandibular lateral incisors were divided in 2 groups: the left teeth were irradiated during the orthodontic movements (experimental group), and the right teeth were the control group. All procedures (impression and laser irradiation) were performed under total intravenous anesthesia by injection of a mixture of xylazine 2% (0.15 mg/kg) and ketamine 10% (10 mg/kg); the dosage was calculated for each dog separately to prevent untoward side effects. The dogs’ monitoring during the procedures was done with control of temperature, pulse rate, and respiratory rate. The animals were also wrapped in quilts to keep them warm in the recovery room after each procedure and properly monitored. During the study, factors such as weight loss and mood change of the dogs were looked for as signs of an adverse reaction to the general anesthesia. No such reactions were noticed in any dog; therefore, it was deduced that the beagles could well withstand several general anesthesia sessions in 4 months.
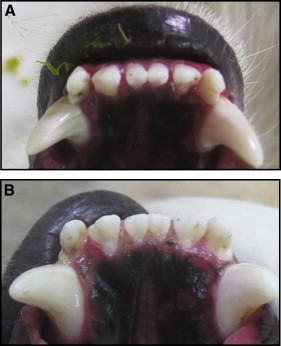
To induce the rotational movement, couple forces were applied to the mandibular lateral incisors on both sides. Orthodontic buttons (American Orthodontics, Sheboygan, Wis) were bonded to the labial and lingual surfaces of the lateral incisors, the labial surfaces of the canines, and the lingual surfaces of the central incisors. Then 2 rings of elastic chain (American Orthodontics) that were able to exert a force of 50 g were engaged between the buttons of the buccal sides of the lateral incisors and the canines. Because of the small size and tight proximity of the lateral and central incisors, a single ring of an elastic chain was used to create rotational couple forces. To prevent forces more than 50 g, this ring was prestretched before being placed between the lingual buttons ( Fig 1 ). The measurements were made with a Correx gauge (Dentaurum, Ispringen, Germany) with precision down to 5 g. The elastic chains were exchanged once a week; after 4 weeks of rotational forces, all orthodontic appliances were removed, and the teeth were monitored for 3 months to investigate the stability of the movements ( Fig 2 ).
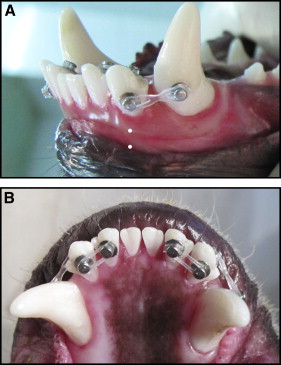
In this study, a gallium-aluminum-arsenide diode laser (DD2; THOR, Chesham, United Kingdom) with a power output of 200 MW and a continuous wavelength of 810 nm (within the infrared range) was emitted from a probe (2 mm in diameter). Irradiation was performed on 2 points at the buccal side of the root of the mandibular left lateral incisor: between the cervical third and the middle third (5 seconds), and between the middle third and the apical third (5 seconds) ( Fig 1 , A ). The probe was placed perpendicular to the tissue with a gentle contact without pressure. Therefore, the tooth received 2 J of energy (200 MW × 10 seconds) during each irradiation session (31.8 J/cm²/point). Laser irradiation was performed on days 0, 1, 2, 3, 4, 7, 14, 21, and 28 after the beginning of force application (9 sessions).
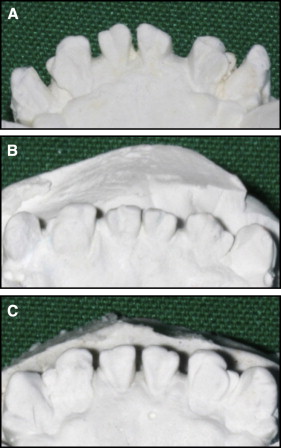
To record the status of the teeth, impressions were taken with silicon materials (Speedex; Coltene/Whaledent, Alstätten, Switzerland) and were poured with stone to be used for designated measurements. The tooth positions were recorded before orthodontic force application (T0); at the end of the fourth week, after the active dental movement phase (T1); at the end of the fifth week, 1 week after stopping the orthodontic force (T2); at the end of the second month, 1 month after stopping the orthodontic force (T3); and at the end of the fourth month, 3 months after stopping the orthodontic force (T4) ( Fig 3 ).
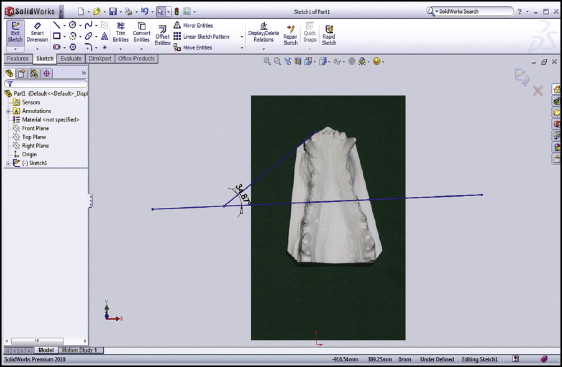
The dental casts were trimmed so that the occlusal surface of the posterior teeth was parallel to the horizon. The photographs with constant magnification were prepared from the occlusal view of the dental models in a background with proper contrast. The digital images were then converted into PSD (photoshop data file) format with Photoshop (version 8; Adobe, San Jose, Calif), and related measurements were made with software (Premium 2010; Dassault Systèmes SOLIDWORKS, Waltham, Mass). In doing so, images were opened in sketch mode, and 3 lines were drawn.
- 1.
A line crossing the most prominent cusp tip of the second premolars on both sides. In case of an abrasion on the second premolar cusp tip, the center of the abraded area was used as the reference to draw this line.
- 2.
A line tangent to the incisal edge of the right lateral incisor.
- 3.
A line tangent to the incisal edge of the left lateral incisor.
Then, using the Extend Entities item from the Trim Entities menu, the second and the third lines were extended until they crossed the first line. Using the Smart Dimension item, the angle between the first and second lines and the angle between the first and the third lines were measured up to 7 decimal places. These numbers were then rounded to 2 decimal places ( Fig 4 ).
The degree of relapse is defined as the amount of tooth movement from its original position in a given time expressed in degrees. The percentage of relapse is the amount of relapse of each tooth to its original position expressed in degrees, divided by the total rotational movement of the tooth in the T0-to-T1 interval, and multiplied by 100.
At the end of the study, to determine the accuracy and reproducibility of the measurements, 30 dental casts were randomly selected using the chart of random numbers, and all measurements were repeated under similar conditions.
Statistical analysis
Means and standard deviations were used to describe the data. Repeated-measures analysis of variance (ANOVA) was used for testing the effects of time and group on the degree of relapse and the percentage of relapse with a significance level of 0.05 ( P ≤0.05). For comparison of the amounts of tooth movement (T0-T1) and tooth relapse between the LLLT and control groups in each time interval, the parametric t test was used. The Bonferroni correction was considered for multiple testing of relapse ( P ≤0.017). To estimate the error of the measurements, Dahlberg’s formula was used,
in which D indicates the difference between 2 measurements, and N indicates the number of measurements. Measurement reliability was measured using the intraclass correlation coefficient (ICC), and the Kolmogorov-Smirnov test was carried out to test the normality of data. All statistical analyses were carried out with the Statistical Package for Social Sciences (version 19; IBM, Armonk, NY).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


