Introduction
The purpose of this study was to evaluate the effects of longitudinal flutes on miniscrew implant (MSI) stability and bone healing.
Methods
Using 11 skeletally mature New Zealand white rabbits, we placed 31 longitudinally fluted and 31 nonfluted, 3-mm-long MSIs in standardized positions in their calvaria and immediately loaded them with 100 g using nickel-titanium coil springs. Insertion torque values were obtained for each MSI placed; removal torque values were obtained for 28 MSIs that had been in place for 6 weeks and 20 MSIs that had been in place for 2 weeks. The bone volume fractions at 6 to 24, 24 to 42, and 42 to 60 μm from the MSI surfaces were evaluated using microcomputed tomography with an isotropic resolution of 6 μm.
Results
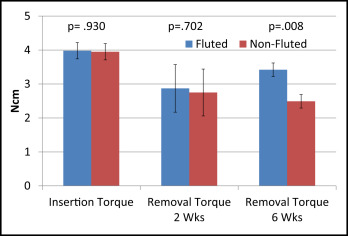
The success rate was 97% for both the fluted and nonfluted MSIs. The difference in insertion torque between the fluted and nonfluted MSIs was not statistically significant ( P = 0.930). After 2 weeks, there was no statistically significant ( P = 0.702) difference in removal torque between the fluted and nonfluted MSIs. After 6 weeks, removal torque values were significantly ( P = 0.008) higher for the fluted (3.42 ± 0.26 N.cm) than the nonfluted (2.49 ± 0.20 N.cm) MSIs. Bone volume fractions of the 6-to-24–, 24-to-42–, and 42-to-60–μm layers were significantly ( P <0.05) greater for the nonfluted than the fluted MSIs.
Conclusions
Loaded 3-mm-long MSIs with and without flutes have high success rates. Longitudinal flutes placed in 3-mm MSIs increased their removal torque by 37% and decreased the amount of bone immediately surrounding them.
Highlights
- •
Loaded 3-mm miniscrew implants (MSIs) placed in animal models can have very high (97%) success rates.
- •
Miniscrews can be stable even when placed with maximum insertion torque values below recommended levels.
- •
Adding flutes to 3-mm MSIs increases the removal torque by 37% after 6 weeks of healing.
- •
There was less bone 6 to 24 μm from the MSI surface than at 24 to 42 or 42 to 60 μm from the implant surface.
- •
There was more bone surrounding nonfluted than fluted MSIs after 2 and 6 weeks of healing.
Miniscrew implants (MSIs) have rapidly gained popularity and acceptance owing to their versatility, minimal invasiveness, low costs, and patient acceptance. Although implant failure remains a major deterrent for many orthodontists, stability rates have been improving. Early systematic reviews reported failure rates between 15% and 20% ; a more recent meta-analysis based on almost 5000 MSIs placed in 2281 patients reported an overall failure rate of 13.5%.
Size poses another limitation to MSI use. Whereas longer MSIs exhibit greater primary stability (greater insertion torque and pullout forces), clinical studies have shown no significant effect of MSI length on success. If size could be decreased, the risk of root injuries during and after insertion could be minimized. A decreased risk of root damage might be expected to shorten treatment times because teeth would not need to be separated. In addition, shorter MSIs require significant less insertion torque than do longer MSIs; this should produce fewer and less extensive microfractures. Less bone damage should decrease healing times.
Even though shorter MSIs confer less primary stability than longer screws, they provide adequate primary stability for forces typically used by orthodontists. Experimentally, 3-mm MSIs loaded with orthodontic forces have been shown to remain stable 91.4% (193 of 212 MSIs) of the time. Although 3-mm MSIs provide only 30% as much holding power as 6-mm MSIs, more than 6.7 kg of force is required to pull them out of 1-mm-thick cortical bone. Moreover, the holding power of shorter MSIs can be improved by 15% to 27% by increasing their outer diameter. Longitudinal flutes also increase the primary stability of shorter MSIs by 7% to 8%. However, these effects were tested in synthetic and cadaver bones; further research is needed to evaluate their effects on secondary stability in living bone.
The purpose of this in-vivo study was to evaluate the effects of longitudinal flutes placed in 3-mm-long MSIs on bone healing and stability. MSI failure rates, insertion and removal torque values, and the quality of bone surrounding the MSIs were evaluated.
Material and methods
Eleven skeletally mature female New Zealand white rabbits, 7 to 8 months of age, were used in this study. The Institutional Animal Care and Use Committee at Texas A&M University Baylor College of Dentistry in Dallas approved the care of the animals and the experimental protocol. Each of the 62 miniscrews placed was subjected to a constant force of 100 g.
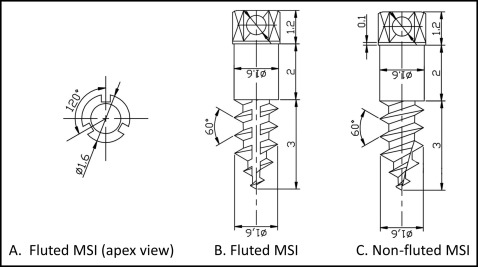
Two miniscrews were specifically fabricated for this study. They were identical except for the flutes that extended down the entire length of the experimental MSI shaft ( Fig 1 ). Each experimental MSI had 3 flutes that were 0.225 mm deep and spaced approximately 120° apart. All MSIs were self-drilling and made of titanium alloy; they were all 3 mm long, with a 1.6-mm outer diameter, and they all had the same thread count and pitch (0.5 mm).
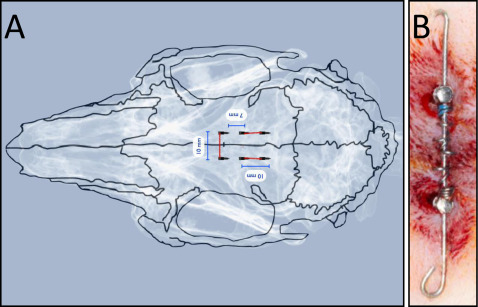
Six MSIs were inserted in each rabbit’s calvaria adjacent to the midsagittal cranial suture ( Fig 2 ). The MSIs were always loaded as pairs. One anterior pair of MSIs was placed transversely across the midsagittal suture. Two additional pairs of posterior MSIs were placed on each side of the midsagittal suture. MSIs were randomly assorted so that when one member of the pair was fluted, the other member was nonfluted, and fluted and nonfluted MSIs were always across the midsagittal suture from each other. Because of its similar blood supply and limited bone marrow, rabbit cranial bone resembles human mandibular bone.
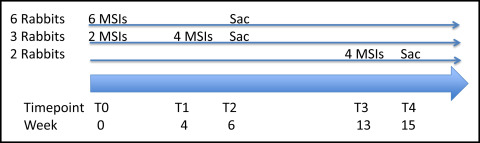
Six rabbits had all 6 MSIs placed at baseline ( Fig 3 ). Three rabbits had the 2 anterior MSIs placed at baseline and the 4 posterior MSIs placed 4 weeks later. Two rabbits had the 2 anterior MSIs placed at baseline and the 4 posterior MSIs placed at week 13. Nine rabbits were euthanized at 6 weeks, and 2 rabbits were euthanized at 15 weeks. Overall, 42 MSIs were loaded for 6 weeks, and 20 MSIs were loaded for 2 weeks.
At the day of MSI placement, the animals were weighed and then sedated with ketamine (75 mg/kg intramuscularly) and xylozine (1 mg/kg). The surgical sites were shaved and disinfected, and the rabbits were anesthetized with 2% lidocaine containing 1:100,000 epinephrine. A 3.0-mm tissue punch was used to prepare the sites. The 2 anterior MSIs were placed 5 mm on each side of the midsagittal suture, approximately in the center of the anteroposterior length of the orbits. A 20-mm-long, 0.020-in-diameter stainless steel guide wire was engaged into eyelets on the MSI heads. The wires were placed through 15-mm-long nickel-titanium open-coil springs, which were compressed between the MSIs to deliver 100 g of continuous forces. The ends of the stainless steel wire were bent, and composite was bonded to the ends to prevent irritation. Gut suture (5-0) was used to close the surgical tissue punch sites. The 4 posterior MSIs were placed 7 mm posterior to the first pair and 10 mm apart from each other. The same 20-mm-long guide wire and 15-mm-long nickel-titanium open-coil springs were used to deliver 100 g of force.
All screws were placed initially with a manual driver leaving 2 or 3 threads visible and then tightened continuously with a static torque screwdriver (Mecmesin, Slinfold, West Sussex, United Kingdom) with a custom adaptor until they were fully inserted and the eyelet holes were aligned. The highest torque value registered during insertion was recorded.
The animals were euthanized with 2 mL of Beuthanasia-D given in the heart and perfused with 1 to 2 L of normal saline solution followed by 1 L of 70% ethanol. Removal torque values of 14 randomly selected pairs of MSIs that had been loaded for 6 weeks were recorded immediately after the animals were euthanized, while still intact in the cranium, using the same screwdriver. The highest removal torque value for each MSI was recorded.
The remaining MSIs were grossly sectioned from the cranium bloc using a fine circular saw. Bone-implant specimens were later refined using a Marathon (Saeyang, Korea) handpiece with a diamond disc under copious irrigation to ensure their passive fit into 9.8-mm-inner-diameter cylindrical specimen carriers for microcomputed tomography scanning.
Removal torque values of the remaining 6-week MSIs and all 2-week MSIs were recorded after the MSIs had been scanned for microcomputed tomography analysis. Each bone-implant specimen was embedded firmly into die-stone plaster. Die-stone plaster surrounded the bone section on all sides but did not cover the top or interfere with the implant bone interface.
The samples were radiographically evaluated using microcomputed tomography (μCT 35; SCANCO Medical, Brüttisellen, Switzerland) with an isotropic resolution of 6 μm. X-ray energy levels were set to 70 kVp, current to 114 μA, and integration time to 800 ms. Bone-implant specimens (maximum of 5) were placed in each holder, along with 4% paraformaldehyde. A scout view was used to visually confirm that the specimens were in the tube before the full scan. A 0.5-mm aluminum filter and a high resolution setting of 1000 projections per 180° were used to ensure high-quality scans with minimal metal implant artifacts.
A volume of interest of each specimen was defined as an approximate circle, with the implant at the center. The coronal limit of the volume of interest was visually defined as the slice at which bone was observed completely surrounding and contacting the MSI. The apical limit of the volume of interest was set to the tip of the MSI. After scanning, a threshold was determined based on multiple specimens to distinguish the MSI from mineralized bone and background space. The threshold used for bone (the gray-scale “brightness” numbers above which all voxels were considered to be bone, and below which all voxels were considered nonbone) had a Gauss value of 3, a sharp value of 4, and a segmentation number of 280. The threshold selected for the titanium had a Gauss value of 3, a sharp value of 4, and a segmentation of 650. Three-dimensional images of the bone-implant specimens were reconstructed from the defined threshold parameters. Proprietary programming scripts (Scanco USA, Wayne, Pa) were used to produce and separate the different 3-dimensional voxel zones used in bone-volume to total-volume (BV/TV) analysis.
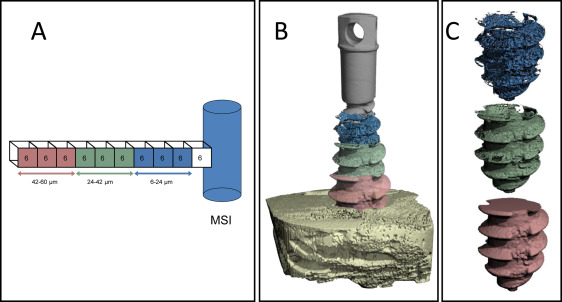
Based on a previously established methodology, the ratio BV/TV was calculated for the 3 layers of bone around the MSIs. Each layer was 3 voxels or 18 μm thick. The layers were defined as 6 to 24 μm, 24 to 42 μm, and 42 to 60 μm from the MSI surface ( Fig 4 ). The 0-to-6–μm layer was excluded because of a possible metallic halation effect.
Statistical analysis
Insertion and removal torque values were normally distributed and analyzed using independent t tests. To standardize the number of slices when evaluating BV/TV, the slice number was divided by the total number of slices, producing relative section thickness ranging from 0% to 100%. Separate analyses were performed for the 2-week and 6-week specimens. Multilevel statistical models were used to determine differences between the fluted and nonfluted MSIs for the 6-to-24–μm, 24-to-42–μm, and 42-to-60–μm layers. Multilevel modeling was chosen because it (1) makes no assumptions as to the intervals used for the independent variable and (2) makes it possible to easily determine the appropriate curves to use and to evaluate group differences.
Results
The overall success rate for the study was 97.0% for the fluted (1 failure out of 31 screws) and 97.0% for the nonfluted (1 failure out of 31) MSIs. Both failures were complete failures; the MSIs were not in bone, and the expansion springs were no longer active. They occurred in different animals and pertained to MSIs loaded anteroposteriorly.
Insertion torque values of the fluted MSIs ranged from 1.5 to 7.0 N.cm, with a mean of 3.98 ± 0.24 N.cm ( Fig 5 ). For the nonfluted MSIs, insertion torque ranged from 1.7 to 6.1 N.cm, with a mean of 3.95 ± 0.24 N.cm. There was no statistically significant ( P = 0.930) difference between the fluted and nonfluted MSIs.