Introduction
Our objectives were to determine whether there are changes on the load deflection rate (L/DP) and the average force (FP) of the superelastic pseudoplateau, and whether permanent deformation is changed in nickel-titanium closed-coil springs (CCSs) after 6 months of clinical use.
Methods
Twenty-two nickel-titanium CCSs (Sentalloy 100 g; Dentsply GAC, York, Pa) were subjected to tensile mechanical testing at 37°C on activations varying from 3.2 to 16.0 mm before and after 6 months of clinical use. A regression line was fitted over the most horizontal area of the unloading part of the stress-strain graph of every CCS, and its slope was used as L/DP. The FP was determined by the midpoint of the longest segment of the curve that could be fit within the regression line with a R 2 of at least 0.999, and permanent deformation was determined graphically by obtaining the strain value when the measured stress reached zero. The data were analyzed by 3 analyses of variance at 2 levels, with 5% of significance.
Results
Time and activation significantly influenced the variables tested ( P < 0.001). Time increased the L/DP and permanent deformation but decreased the FP. Activation decreased L/DP, FP, and permanent deformation. Significant interactions between time and activation were detected for FP ( P = 0.013) and deformation ( P < 0.001).
Conclusions
After 6 months of active clinical use, the analyzed springs had a significant but small increase in their L/DP; FP dropped up to 88%, and the CCSs deformed up to 1.26 mm.
Highlights
- •
We tested nickel-titanium closed-coil springs before use and after 6 months of use.
- •
We examined the slope and force of the pseudoplateau and elastic recovery.
- •
The properties of the springs decayed significantly over time.
- •
Slope increased slightly.
- •
Force decreased up to 88%, and permanent deformation occurred.
Efficient orthodontic space closure must be carefully planned and should be conducted with a known force system. One method of space closure is through sliding mechanics and chain elastics or closed-coil springs (CCSs) of stainless steel or nickel-titanium. The use of nickel-titanium springs has been suggested as an alternative to elastomeric products because they produce faster rates of space closure as a result of the constant forces produced by their superelasticity.
When enough stress is applied to nickel-titanium alloys, it can induce a transformation in its crystallographic structure from an austenitic phase to a martensitic phase, called stress-induced martensite. When a stress-induced martensite transformation occurs and a reverse transformation takes place, upon removal of the stress, a straight and near-flat area (called a pseudoplateau ) occurs on its stress-strain graph; thus, it is said that superelasticity occurred.
During orthodontic treatment, it is desired for a nickel-titanium CCS to be superelastic, producing a low elastic modulus, a mostly constant force, and no deformation. Normally, there should be no concerns about permanent deformations because the literature reports activations of up to 500% of the original length of the CCSs without deformation. However, it is unclear whether CCSs undergo permanent deformation with clinical use, since springs made of other alloys do exhibit stress relaxation.
Despite being nearly constant, the forces generated by nickel-titanium appliances in general may vary over time because of a phenomenon known as stress relaxation. Some authors have observed a time-dependent permanent deformation in nickel-titanium archwires, decreasing the forces produced. It has also been reported that nickel-titanium wires show a higher probability of fatigue and exhibit changes in their surface after clinical use, but changes of their mechanical properties remain controversial. Although 1 in-vitro study and 1 in-vivo study showed that recycled archwires are less superelastic, other in-vitro studies observed no significant differences in mechanical properties. Regarding nickel-titanium CCSs, the authors of several in-vitro studies evaluated the forces produced by them in a simulated oral environment, but similarly, the results are controversial, with increases, decreases, and no differences of the forces over time, suggesting that an in-vivo clinical study is necessary to bring new light to this controversy.
It is clinically important to have as much information as possible on the mechanical properties of nickel-titanium CCSs over time, specifically on the elastic modulus, the average force level used, and the permanent deformation of these devices. This would allow the clinician to know whether a nickel-titanium CCS should be replaced or even whether it could be recycled, but there is no in-vivo research evaluating the effects of time and use on CCSs. Therefore, the aims of this study were to determine the changes that occur in the load-deflection rate of the superelastic pseudoplateau (L/DP), the average force of the superelastic pseudoplateau (FP), and the permanent deformation of nickel-titanium CCSs after clinical use.
Material and methods
The sample for this prospective study was composed initially of 50 nickel-titanium CCSs (Sentalloy 100 g; Dentsply GAC, York, Pa), which were to be used in a randomized clinical trial for canine retraction.
Before clinical use, a mechanical testing machine (DL 2000; EMIC, São José dos Pinhais, Brazil) was used to test the springs to determine their L/DP rates, FP, and permanent deformation. The springs and the hooks that attached them to the machine were submersed in 37°C ± 1°C of distilled water, which was temperature controlled with a 30-W heater and a thermostat.
The mechanical test activated the springs to 3.2 mm (act1), returning them to their initial position (zero) and then activating them to 6.4 mm (act2), 9.6 mm (act3), 12.8 mm (act4), and finally 16.0 mm (act5), always returning to the initial position between activations.
To ensure correct activations, any possible initial looseness of the springs was avoided by adjusting them in increments of 0.1 mm manually with the digital indicator of the testing machine before the test started. The software Tesc (version 3.04; EMIC) recorded all force values during the test, expressed in raw data format at a rate of 20 mm per minute. No spring showed permanent deformation after the tests. They were properly identified so that the values of the first (T1) and second (T2) tests, made after clinical use, would correspond to the same springs.
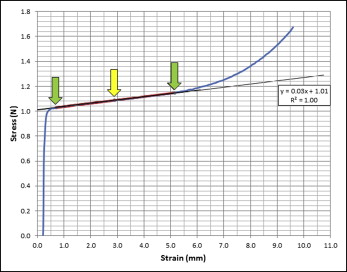
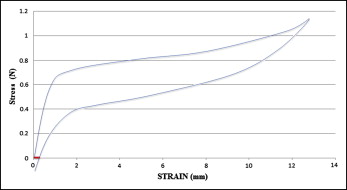
To collect the variables, stress raw data of each spring were exported to Excel (Microsoft, Redmond, Wash). A linear regression was fitted in the most horizontal area of the stress-strain graph on deactivation to allow the determination of the superelastic pseudoplateau. Two points were chosen to determine the beginning and the end of the pseudoplateau, which was the longest segment of the stress-strain graph explained by the regression line, with a coefficient of determination not less than 0.999. The modulus of elasticity of the superelastic pseudoplateau (L/DP) was determined by the slope of the regression line ( Fig 1 ); FP was determined by the midpoint of the superelastic pseudoplateau; and permanent deformation was determined graphically at each stress-strain curve by obtaining the deflection value (variable x) when the amount of force (variable y) reached zero ( Fig 2 ).
The 50 CCSs tested were then used for canine retraction in 25 patients. They were activated by 17 mm (twice the total length of 8.5 mm) and were reactivated to the same length every month. After 6 months of treatment, 22 springs were selected for a second test, which was carried out with the same parameters as the first. Only 22 springs were tested because the remaining springs were still in use in the clinical trial after 6 months. The 22 springs used for the test at T2 showed no visible signs of permanent deformation after clinical use.
Because the data collected before and after treatment were normally distributed, the SPSS statistical software (version 16.0; SPSS, Chicago, Ill) was used to perform 3 analyses of variance (at 2 levels), with a significance level of 5%. The tests were used to determine differences between times and activations, as well as to identify a possible interaction between these 2 factors in the variables L/DP, FP, and permanent deformation.
Results
Clinical use (time) significantly influenced the L/DP of the springs ( P < 0.001; Table I ). When their total profile was evaluated, the average L/DP increased from T1 (0.42) to T2 (0.53). Activation also influenced L/DP ( P < 0.001; Table II ). The Tukey post hoc test showed that L/DP values were different at act1 (0.11 N/mm) and act2 (0.05 N/mm), but they were the same at act3 (0.03 N/mm), act4 (0.02 N/mm), and act5 (0.02 N/mm) ( Table II ). No interaction was detected between time and activation in L/DP ( P = 0.721).
| Group | L/DP (SD) | FP (SD) | Deformation (SD) |
|---|---|---|---|
| T1 | 0.42 (0.04) | 1.06 N (0.07) | 0.22 mm (0.13) |
| T2 | 0.53 (0.04) | 0.16 N (0.11) | 1.15 mm (1.32) |
| P | <0.001 | <0.001 | <0.001 |
| Activation | L/DP (SD) | FP (SD) | Deformation (SD) |
|---|---|---|---|
| Act1 (3.2 mm) | 0.11 A (0.02) | 0.61 N A (0.49) | 0.28 mm A (0.24) |
| Act2 (6.4 mm) | 0.05 B (0.02) | 0.62 N A (0.47) | 0.49 mm AB (0.44) |
| Act3 (9.6 mm) | 0.03 C (0.01) | 0.61 N A (0.46) | 0.61 mm AB (0.65) |
| Act4 (12.8 mm) | 0.02 C (0.01) | 0.65 N A (0.44) | 0.84 mm BC (1.00) |
| Act5 (16.0 mm) | 0.02 C (0.01) | 0.54 N B (0.44) | 1.26 mm C (1.82) |
| P | <0.001 | <0.001 | <0.001 |
Time significantly influenced the FP when the overall profile of the springs was evaluated ( P < 0.001; Table I ), with FP decreasing from T1 (1.06 N) to T2 (0.16 N) ( Table I ). Activation also significantly affected the FP ( P < 0.001; Table II ). The means of the FP were equal in act1 (0.61 N), act2 (0.62 N), act3 (0.61 N), and act4 (0.65 N), decreasing in act5 (0.54 N) ( Table II ). A significant interaction was found between the activation and time factors in variable FP ( P = 0.013 and P < 0.001, respectively).
Time influenced significantly the permanent deformation of the springs ( P < 0.001; Table II ). When the springs were evaluated for deformation, the total permanent deformation increased from T1 (0.22 mm) to T2 (1.15 mm) ( Table I ). Permanent deformation was also influenced by activation ( P < 0.001; Table II ), with values gradually becoming different from 0.28 mm at act1, 0.49 mm at act2, 0.61 mm at act3, 0.84 mm at act4, and up to 1.26 mm at act5 ( Table II ). A significant difference was also detected between time and activation in the variable of permanent deformation ( P < 0.001).
Results
Clinical use (time) significantly influenced the L/DP of the springs ( P < 0.001; Table I ). When their total profile was evaluated, the average L/DP increased from T1 (0.42) to T2 (0.53). Activation also influenced L/DP ( P < 0.001; Table II ). The Tukey post hoc test showed that L/DP values were different at act1 (0.11 N/mm) and act2 (0.05 N/mm), but they were the same at act3 (0.03 N/mm), act4 (0.02 N/mm), and act5 (0.02 N/mm) ( Table II ). No interaction was detected between time and activation in L/DP ( P = 0.721).
| Group | L/DP (SD) | FP (SD) | Deformation (SD) |
|---|---|---|---|
| T1 | 0.42 (0.04) | 1.06 N (0.07) | 0.22 mm (0.13) |
| T2 | 0.53 (0.04) | 0.16 N (0.11) | 1.15 mm (1.32) |
| P | <0.001 | <0.001 | <0.001 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


