Introduction
The goal of this study was to modify the transpalatal arch design that is used for vertical control of the molars, based on individual muscle strength and morphology features of the tongue during swallowing.
Methods
Individual Silastic (Müller-Omicron, Cologne, Germany) swallowing tongue records were created and measured for 32 healthy volunteers. The transpalatal arches were modified by adding acrylic pads, based on the swallowing tongue records. Tongue pressure exerted on the hard palate and the acrylic pads at 3 distances to the palatal mucosa during swallowing was measured by pressure sensors for 18 subjects.
Results
The intraclass correlation coefficient of the thickness of swallowing tongue records taken by 2 researchers was 0.977, indicating good consistency between these researchers. A significant negative correlation was found between the thickness of the swallowing tongue records and individual tongue pressure (r = −0.511; P <0.01). Tongue pressure exerted on the fabricated pads consistent with swallowing tongue records was significantly higher than on the hard palate, yet not significantly higher than tongue pressure exerted on the pads positioned 3 mm closer to the palatal mucosa. In contrast, increasing the distance of the pad 3 mm away from the mucosa led to significant augmentation of tongue pressure.
Conclusions
Creating patient swallowing tongue records is a repeatable and reliable method to reflect individual differences in morphologic features and muscle strengths of the tongue. Decreasing the distance of the pads to the mucosa is preferable if a high force to intrude molars will not be used. On the premise of a patient’s tolerance, increasing the distance of the pads away from the mucosa leads to augmentation of tongue force.
Highlights
- •
Silastic swallowing tongue records were created for 32 subjects.
- •
Transpalatal arches were modified by adding acrylic pads, based on the swallowing tongue records.
- •
Tongue pressure on the pads was significantly higher than on the hard palate.
- •
Move pads closer to mucosa if high force to intrude molars is not expected.
- •
Moving the pads away from the mucosa leads to augmentation of tongue force.
The vertical control of molars is a current but also difficult issue in common orthodontic treatment because extrusion of teeth is much easier and more likely to happen than intrusion. Molar extrusion may cause adverse effects such as open bite, downward-backward rotation of the mandible, increased lower anterior face height, and impaired facial harmony. In contrast, molar intrusion is deemed to be an efficient treatment for an open bite and is effective for anteriorly rotating the mandible to improve the facial profile, especially in hyperdivergent Class II patients.
The most commonly used devices to control vertical dimensions are the high-pull headgear and the transpalatal arch (TPA). However, their effectiveness has not been demonstrated in clinical studies. A temporary anchorage device is the only method that is commonly accepted with regard to the absolute intrusion of molars, and it was also used in a modified TPA by some researchers. Yet, not all patients or orthodontists can accept this method for treatment because of the potential risks. A reliable conservative technique is necessary for this condition.
Some researchers tried to change the position or the design of the TPA to make it more effective for molar intrusion. Chiba et al measured the pressure of the tongue on the TPA and found that different pressures could be acquired by changing the vertical or sagittal position of the TPA. They speculated that more precise use of the TPA would allow the expected treatment goals to be achieved. In the research of Wise et al, mean molar extrusion was 0.2 mm less in the TPA group. Despite the statistical insignificance, they speculated that the intrusion effect of the TPA would be enhanced if its distance to the palatal mucosa was increased, or if its interactional area with the tongue was augmented by adding an acrylic plate to the loop. Based on this hypothesis, DeBerardinis et al used a modified TPA by adding an acrylic plate and named it a vertical holding appliance (VHA). A retrospective clinical study was carried out that indicated that the VHA was significantly more useful in restricting and even helping to reduce the percentage of lower anterior vertical face height than the Tweed technique. The VHA was also thought to have an effect of distally moving the maxillary molars because the tongue moved forcibly upward and also backward toward the hard palate during swallowing, and it was successfully used in a nonextraction Class II patient.
The position and the shape of the added acrylic plate were considered to be the most important features of the VHA, based on clinical experience. The acrylic plate has been ambiguously described as dime-sized, at the level of the gingival margin of the molar bands. Based on related studies, there are large individual differences in tongue pressure exerted on both the hard palate and the TPA among different subjects. Tongue surface morphology during swallowing exercises was also different. Patients’ comfort and tongue force level on the VHA may also be questionable. Our study focused on further modifying the design of the TPA that is used for vertical control of molars by the new method of taking Silastic (Müller-Omicron, Cologne, Germany) swallowing tongue records, so that a modified TPA could be created based on a patient’s individual muscle strength and tongue morphology features during swallowing. In addition, tongue pressure exerted on the hard palate and the acrylic pads of the modified TPA positioned at different distances from the mucosa was measured and compared to offer a reference for the adjustment of intrusive force in future clinical research so that we could obtain the specific treatment outcome that we expected, as well as better comfort for and compliance of patients.
Material and methods
The subjects of our study consisted of 32 healthy volunteers (9 men, 23 women; age range, 23-37 years; mean, 28.6 ± 3.6 years) with no disturbance of deglutition, abnormality in the number or position of teeth except for the third molar, history of orthodontic treatment and temporomandibular disorders, and abnormality in occlusion. Written informed consent was obtained from each subject after explanation of the aim and methodology of the study. The study was approved by the institutional review board of Peking University School and Hospital of Stomatology (PKUSSIRB-2013056).
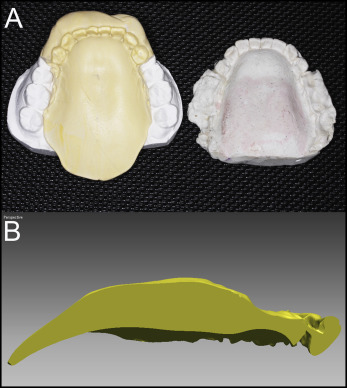
To create a swallowing tongue record, we had each subject sit on the chair in a 45° oblique position, where a defined amount (a spoonful) of Silastic impression material (betasil putty soft; Müller-Omicron) was placed on the hard palate to obtain an impression of the tongue during dry swallowing. Thus, we recorded the morphologic feature and position of the tongue during the swallowing exercise in that condition. These impressions were referred to as the swallowing tongue record. Negative molds were made with plaster using these Silastic records ( Fig 1 ). Two researchers (K.X. and J.Z.) took swallowing tongue records for each subject at different times and measured the thickness of the Silastic tongue records on the midpoint of the line drawn from the lingual grooves of the 2 maxillary first molars.
Adams clasps rather than molar bands were used as the retention part of the modified TPA for the convenience of the experiment. In addition, a framework for the acrylic pads was constructed of 0.9-mm stainless steel wire. The framework of Adams clasps bestriding the contact area of the teeth would provide a vertical “stop” effect when the whole appliance was pressed gingivally by the tongue and help to measure the exact pressure magnitude. The palatal acrylic pads were made by first creating a negative plaster mold of a swallowing tongue record occluded with the maxillary cast to shape the resin before it polymerized. This allowed for the distance from the mucosa to the acrylic pad to be identical to that of the impression of the tongue position cast. In addition, the lingual surface of the pad was made according to the functional morphologic features of the tongue ( Fig 2 ). In addition to the one created according to the thickness of the swallowing tongue record (referred to as 0 mm), 2 additional modified TPAs were also created for each subject: with the distances of the acrylic pads to the mucosa from the original swallowing tongue records set at −3 mm and +3 mm. Next, the pads were trimmed to an appropriate and individualized size. The width of the pads was about two thirds of the molar-to-molar distance. The anterior edge of each pad was at the level of the mesial aspect of the first molars, and the posterior edge was to the distal aspect of the second molars.

For the tongue pressure analysis system and measurement, we used sensors used in this research (FSR 400; Interlink Electronics, Westlake Village, Calif), a type of resistance pressure transmitter. The data acquisition unit and the data analysis software were fabricated and calibrated.
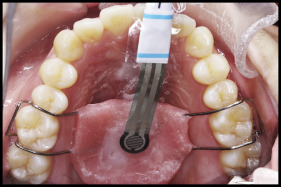
Before the measuring, all subjects wore the modified TPA for 10 minutes to adapt to the appliance and to minimize the influence of oral temperature. Tongue pressure production during swallowing saliva was recorded with the subjects sitting in a chair in a 45° oblique position. The sensors were attached to the palatal mucosa on the midpoint of the line drawn from the lingual grooves of the 2 maxillary first molars and the center of the functional surfaces of the acrylic pads, positioned at different heights using denture adhesive material (Touch correct II; Shionogi, Osaka, Japan) ( Fig 3 ). During the measurement of tongue pressure, the sensor was tightly fitted to the palate and the pad, and the subject could bite and swallow saliva with minimal discomfort because of its thinness and flexibility. At the recording time, the subject was given the signal to swallow. The maximum tongue pressure of each measuring point was evaluated from the waveform of each recording ( Fig 4 ). At least 8 replicates were taken for each recording time, and mean swallowing pressures for the different positions (+3, 0, and −3 mm) were computed and summarized for all subjects.

Statistical analysis
All data were analyzed using SPSS software (version 19.0; IBM, Armonk, NY). Intraclass correlation coefficients were used to evaluate the repeatability and reliability of the method for taking individual swallowing tongue records. The Pearson coefficient was used to evaluate the correlation between the thickness of the swallowing tongue record and the pressure of the tongue on the hard palate. All data were determined to have normal distributions as assessed with the Kolmogorov-Smirnov test. Mean comparisons of tongue pressure exerted on the hard palate and on the acrylic pads of the different vertical positions were conducted with single-factor variance analysis, and the pairwise comparison was performed with the least significant difference method.
Results
The intraclass correlation coefficient of the thickness of the 2 Silastic swallowing tongue records on the midpoint of the 2 maxillary first molars taken and measured by the 2 researchers for each subject was 0.977, indicating good consistency. Means and the variability of the thickness of the Silastic swallowing tongue records and the tongue pressure exerted on the hard palate during swallowing by the 32 subjects for the correlation analysis is shown in Table I . Measurements of tongue pressure exerted on the acrylic pads at different distances to the palatal mucosa were completed in 18 subjects ( Table II ). A significant negative correlation was found between the thickness of the Silastic swallowing tongue records and the tongue pressure exerted on the hard palate during swallowing of saliva without an intraoral appliance (r = −0.511; P <0.01) ( Fig 5 ).
| Mean and SD | Minimum | Maximum | 95% CI | |
|---|---|---|---|---|
| Record thickness | 9.35 ± 1.77 | 6.35 | 12.9 | 8.67, 9.93 |
| Tongue pressure | 4.74 ± 1.48 | 1.89 | 8.24 | 4.21, 5.27 |
| Subject | Hard palate | Tongue record, −3 mm | Tongue record, 0 mm | Tongue record, +3 mm |
|---|---|---|---|---|
| 1 | 2.18 | 2.88 | 3.11 | 3.59 |
| 2 | 4.62 | 5.24 | 5.51 | 8.3 |
| 3 | 2.83 | 5.67 | 6.44 | 6.18 |
| 4 | 4.2 | 3.05 | 3.12 | 4.02 |
| 5 | 4.48 | 3.82 | 3.95 | 4.66 |
| 6 | 5.84 | 6.96 | 7.43 | 9.83 |
| 7 | 4.06 | 3.28 | 4.6 | 4.8 |
| 8 | 4.34 | 2.16 | 2.8 | 2.65 |
| 9 | 5.52 | 5.62 | 7.48 | 11.35 |
| 10 | 4.78 | 5.12 | 6.37 | 6.25 |
| 11 | 5.81 | 6.68 | 7.62 | 8.61 |
| 12 | 1.89 | 4.21 | 6.54 | 9.71 |
| 13 | 5.73 | 6.53 | 6.57 | 10.9 |
| 14 | 6.02 | 7.58 | 5.29 | 9.62 |
| 15 | 5.96 | 5.19 | 9.44 | 12.33 |
| 16 | 3.37 | 8.23 | 5.97 | 11.14 |
| 17 | 7.36 | 8.22 | 10.67 | 11.07 |
| 18 | 5.41 | 6.06 | 6.08 | 7.49 |
| Mean | 4.69 ± 1.44 | 5.23 ± 1.70 | 6.18 ± 2.16 | 7.91 ± 3.05 |
| 95% CI | 3.67, 5.41 | 4.39, 6.08 | 5.10, 7.26 | 6.40, 9.45 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


