Introduction
Disc displacement (DD) is common in adolescents, but not much is understood about its cause. Assessment of the directionality of incipient DDs may provide clues about the etiology.
Methods
The sample consisted of magnetic resonance images of 143 temporomandibular joints with incipient DD from 89 preorthodontic patients (mean age, 10.8 years). The severity of DD was evaluated by grading the degree of displacement depicted in the images in the sagittal and coronal planes, and each incipient DD was categorized based on the directionality.
Results
Of the 143 incipient DDs, rotational anterolateral DD (43.36%) and partial anterior DD in the lateral portion (27.27%) were the most common; rotational anteromedial DD (9.09%) and partial anterior DD in the medial portion (1.40%) accounted for only 10.49%. Anterior DD was seen in 12.59%. Pure sideways shift was rare; lateral DD was seen in 2.80%, and medial DD in 3.50%. Thus, the lateral part of the joint was involved in a majority of the incipient DDs and the medial part far less. No sex difference was noted in this trend, but the difference between the right and left sides was statistically significant.
Conclusions
These results indicate a predilection for the lateral part of the joint in incipient DDs and may have etiologic implications.
Highlights
- •
Directional characteristics of incipient disc displacements were analyzed with MRI.
- •
Most incipient disc displacements involved the lateral aspect of the TMJ.
- •
No posterior disc displacement was observed in this sample.
- •
The difference between the right and left joints was statistically significant.
- •
Higher frequency of displacements with a lateral component was seen in left TMJs.
The articular disc of the temporomandibular joint (TMJ) plays a vital role in the development and function of the TMJ. When the disc is not interposed between the condyle and the articular eminence in what has been considered a more normal anatomic relationship, the condition can have deleterious effects, particularly in growth and development. Studies have evaluated the different imaging modalities available to visualize the TMJ and have advocated magnetic resonance imaging (MRI) as the prime diagnostic method because of its ability to accurately depict the disc position in sagittal and coronal images. In 1 MRI study, none of the 60 TMJs of infants and young children up to age 5 years examined had disc displacement (DD). Thus, the study suggested that DD is not a congenital phenomenon but, rather, an acquired condition. In addition, research has consistently shown that DD is not rare in asymptomatic populations, with a prevalence of approximately 30%, and that the young adolescent population is not an exception to this phenomenon. The peak incidence of symptomatic DD has been shown to be during puberty in both boys and girls, making the adolescent population at risk for developing TMJ dysfunction symptoms.
An important question is why and how DD occurs. Several possible etiologic factors have been proposed, but no definitive answer is available at this time. It is apparent, however, that the etiology of advanced DD is usually multifactorial, making establishment of cause-and-effect relationships difficult. Previous reports of the relatively higher frequency of anteromedial DD explained it by the pulling forces of the lateral pterygoid muscle. However, several recent studies have shown that anterolateral displacement is more frequent. Although MRI evaluation of early DD can be valuable in showing how DD starts—which in turn may provide important clues about its etiology—early DD has not been studied.
The purpose of this study was to determine any tendency in the direction of early DD. The data were retrospectively analyzed using available MRIs of a young preorthodontic population with incipient DD.
Material and methods
The study sample was derived from a population of 153 consecutive preorthodontic patients who had MRIs of their TMJs taken for evaluation of disc status. In a previous study, all MRIs were evaluated by 2 calibrated investigators, and each TMJ disc was categorized as normal or as 1 of the 4 stages of DD based on the severity of displacement. The study sample consisted of 143 TMJs from 89 preorthodontic patients (35 boys, 54 girls) who were determined to have incipient DD in the previous study. The patients ranged in age from 7 to 15 years, with a mean age of 10.8 years. Because the MRIs were taken before this retrospective study for diagnostic purposes, the patient data were anonymous to the researchers, and our summarized findings in this study are incidental, the ethical board did not require approval for this study.
All scans were done at 1 clinic by the same technician using the 1.5-T MRI system (Gyroscan ACS-NT Intera; Philips, Amsterdam, The Netherlands) with surface coils. The images were taken in the oblique sagittal plane and the oblique coronal plane with the subject in closed-mouth and open-mouth positions. Open-mouth sagittal images were obtained using mouth pieces set at 10 mm below maximal voluntary incisal opening. Proton density-weighted images were taken with a 2.5-mm-section thickness, a 12-cm field of view, a repetition time of 2500 ms, an echo time of 20 ms, and a 256 × 256 measurement phase scanning matrix.
MRIs of the 143 TMJs were previously evaluated by 2 investigators for anterior or posterior displacements in the sagittal planes and medial or lateral displacements in the coronal planes using a standardized grading system, which enabled categorization of the TMJs into normal and 4 stages of DD based on the severity of the displacement.
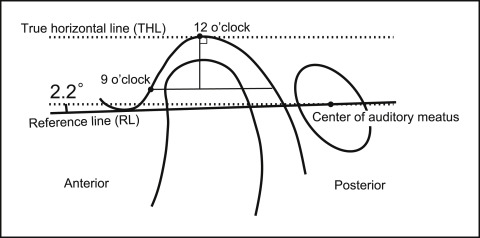
In the sagittal plane, a method described by Ikeda was used to establish the 12 o’clock mark as a reference point from which to evaluate the severity of DD ( Fig 1 ). A reference line was drawn connecting the most inferior point of the articular eminence and the center of the auditory canal. The reference line was then rotated 2.2° to establish the true horizontal line on the MRIs. The 12 o’clock position is the point at which the true horizontal line is tangential at the deepest point on the glenoid fossa. The 9 o’clock position is where the true horizontal line intersects with the eminence when lowered to the most prominent point on the anterior surface of the condyle. The center of the clock is the intersection of the true horizontal line through the 9 o’clock position with a line perpendicular to the true horizontal line through the 12 o’clock position. The 10 and 11 o’clock positions are determined by dividing the angle between the 9 and 12 o’clock positions into 30° segments.
The position of the posterior margin of the posterior band was evaluated relative to the established 12 o’clock position. Disc position were defined as normal, level 1, level 2, or level 3 when the posterior band was at 12 o’clock, 11 o’clock, 10 o’clock, or 9 o’clock or below, respectively ( Fig 2 ). The position of the disc in each joint was evaluated in 3 sagittal MRI slices (medial, central, and lateral aspects of the joint).
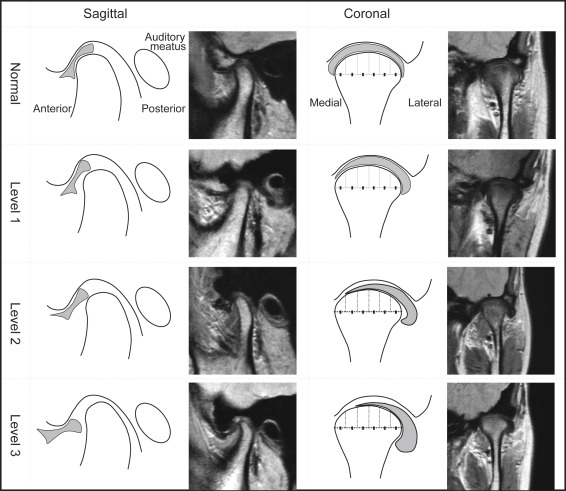
Sideways (mediolateral) DD was evaluated in the coronal plane parallel to the long axis of the condyle and assigned the rating of normal when the disc was centered between the medial and lateral poles. Level 1 was when the disc was markedly thickened on the side to which it was displaced or when the disc was displaced up to a sixth of the mediolateral width of the condyle; level 2 was when the disc was displaced up to a third of the mediolateral width with a drooping look on the displacement side; and level 3 was when the disc was displaced at least half of its mediolateral width ( Fig 2 ).
Based on the disc position assessed by the 4 MRI slices (3 sagittal and 1 coronal), each joint was categorized as normal or as 1 of the 4 stages of DD ( Table I ), ranging in severity from incipient DD to total DD without reduction. We focused on the 143 TMJs that were in the incipient stage of DD (stage 1) when all 3 sagittal slices and the coronal slice show a displacement of level 1 or less.
| Early DD |
| Stage 1 (incipient stage) |
| All 3 sagittal slices and the coronal slice in level 1 or less |
| Stage 2 (partial DD) |
| Stage 2A: 2 of 3 sagittal slices in level 1, and coronal slice in level 1 or less |
| Stage 2B: only 1 of 3 sagittal slices in level 1, and coronal slice in level 2 or less |
| Stage 2C: all 3 sagittal slices in level 2 or more, and coronal slice in level 2 or less |
| Advanced DD |
| Stage 3 (total DD with reduction) |
| All 3 sagittal slices in level 3, and coronal slice in levels 1 to 3 with disc reduction on opening |
| Stage 4 (total DD without reduction) |
| All 3 sagittal slices in level 3, and coronal slice in levels 1 to 3 without disc reduction on opening |
Statistical analysis
Each incipient DD was categorized based on the direction of displacement using the classification established in the study by Tasaki et al ( Table II ), and the prevalence percentage of DD by directionality was determined. The data were further analyzed using chi-square tests to detect any statistically significant disparity in the prevalence of the various DDs because of sex or right-to-left differences. Since 2 investigators (R.I. and K.I.) independently evaluated the MRI data, interobserver reliability was determined by calculating the kappa coefficient for their classifications of the entire sample of 143 TMJs with incipient DDs.
| Disc displacement types | Sagittal MRIs | Coronal MRIs |
|---|---|---|
| Anterior | Posterior band of disc anterior to 12 o’clock position in multiple sections | Disc centered between medial and lateral poles in all sections |
| Partial anterior in lateral | Posterior band of disc anterior to 12 o’clock position in lateral section only | Disc centered between medial and lateral poles in all sections |
| Partial anterior in medial | Posterior band of disc anterior to 12 o’clock position in medial section only | Disc centered between medial and lateral poles in all sections |
| Rotational anterolateral | Posterior band of disc anterior to 12 o’clock position in one or more sections | Disc slightly shifted laterally |
| Rotational anteromedial | Posterior band of disc anterior to 12 o’clock position in one or more sections | Disc slightly shifted medially |
| Lateral | Posterior band of disc at 12 o’clock position in all sections | Disc slightly shifted laterally |
| Medial | Posterior band of disc at 12 o’clock position in all sections | Disc slightly shifted medially |
| Posterior | Posterior band of disc posterior to 12 o’clock position in one or more sections | Disc centered or shifted medially/laterally |
Results
In this sample of 143 incipient-stage DDs, no joint had a posterior displacement, but displacements in other directions (anterior, lateral, and medial) were observed. As shown in Figure 3 , A , and Table III , rotational anterolateral DD was the most frequent (62 DDs) and represented 43.36% of the incipient DDs (see Table II for classifications). Partial anterior DD in the lateral portion was the next most common DD (39 DDs, 27.27%). Anterior DD was the third most frequent overall (18 DDs, 12.59%). As previously stated, no posterior displacement was observed in this incipient DD sample, and the prevalence of other displacements (partial anterior in medial, rotational anteromedial, lateral, and medial) was low.
| Disc displacement types | Total | Male | Female | Right | Left |
|---|---|---|---|---|---|
| Anterior (A) | 18 (12.59%) | 5 (8.77%) | 13 (15.12%) | 15 (20.00%) | 3 (4.41%) |
| Partial anterior in lateral (PAL) | 39 (27.27%) | 16 (28.07%) | 23 (26.74%) | 21 (28.00%) | 18 (26.47%) |
| Rotational anterolateral (RAL) | 62 (43.36%) | 27 (47.37%) | 35 (40.70%) | 24 (32.00%) | 38 (55.88%) |
| Lateral (L) | 4 (2.80%) | 1 (1.75%) | 3 (3.49%) | 1 (1.33%) | 3 (4.41%) |
| Medial (M) | 5 (3.50%) | 3 (5.26%) | 2 (2.33%) | 3 (4.00%) | 2 (2.94%) |
| Rotational anteromedial (RAM) | 13 (9.09%) | 4 (7.02%) | 9 (10.47%) | 10 (13.33%) | 3 (4.41%) |
| Partial anterior in medial (PAM) | 2 (1.40%) | 1 (1.75%) | 1 (1.16%) | 1 (1.33%) | 1 (1.47%) |
| Posterior (P) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Total | 143 | 57 | 86 | 75 | 68 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


