Introduction
The mandibular arch form at the levels of both the application point of the orthodontic bracket and the basal bone in adults and children with Class I malocclusion and Class II Division 1 malocclusion was investigated.
Methods
One hundred thirteen pretreatment mandibular casts were scanned to generate a 3-dimensional computer model of each cast. The casts were divided into Class I and Class II Division 1 malocclusion groups, and were further divided into adults (age, ≥25 years) and children (age, ≤18 years). Two reference points, FA and WALA, were assigned for each tooth. The FA and WALA arch forms were compared, and the distances between corresponding points and intercanine and intermolar widths were analyzed.
Results
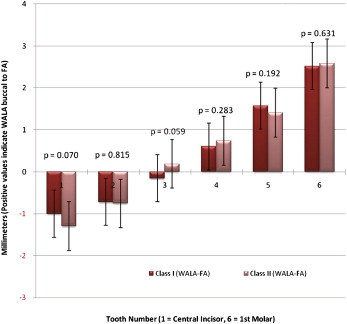
The mandibular intercanine FA point widths were significantly greater in the Class II Division 1 malocclusion group than in the Class I malocclusion group ( P <0.05) and were also significantly greater in the Class I adults than in the Class I children ( P <0.05). Both the canine FA and WALA point distances and the molar FA and WALA point distances were moderately to highly correlated (R 2 >0.55) and highly significant ( P <0.001) for all groups. The FA and WALA curves for all groups had individual differences, especially in the premolar and molar areas.
Conclusions
The Class II Division 1 mandible is essentially the same as the Class I mandible with respect to basal bone and dental arch dimensions. WALA points can be used to predict individual dental arch forms in adults and children. Dental and basal arch forms were not significantly different between adolescents and adults.
Editor’s comment
When in practice, I used to meet periodically with my laboratory personnel to review the cost of our routine supplies: archwires, brackets, and so on. One day after returning from a continuing education course, my laboratory assistant asked why I spent time altering the shape of nearly every archwire placed in a patient’s mouth; after all, they could be purchased in different shapes and sizes for more convenient use without further bending. That got me thinking, and I now realize that several good articles from Harvard University have recently made it easier to understand why most good clinicians bend a new archwire to match the original arch form before placing it in the patient’s mouth. Ronay et al (Ronay V, Miner RM, Will LA, Arai K. Mandibular arch form: the relationship between dental and basal anatomy. Am J Orthod Dentofacial Orthop 2008;134:430-8) used a unique methodology to evaluate mandibular arch forms in 35 Class I patients, and Ball et al (Ball RL, Miner RM, Will LA, Arai K. Comparison of dental and apical base arch forms in Class II Division 1 and Class I malocclusions. Am J Orthod Dentofacial Orthop 2010;138:41-50) used this methodology to evaluate mandibular arch forms in 35 Class II Division 1 patients. The only difference in this current study was that the authors compared the Class I patients with Class II Division 1 patients, and looked at adolescents and adults. The authors concluded that a general arch form cannot be applied to all patients with any malocclusion for any age group. One conclusion of the article by Ronay et al was that “Both FA and WALA point-derived arch forms were individual and therefore could not be defined by a generalized shape.”
The authors of this study were quick to note, “It is true that this study is very similar to those done by Ronay and Ball. However, it was always felt that mixing growing individuals and adults in a sample could be problematic. With growth of the mandible, we were not sure whether the relationship between the dental and bony arches changes, and felt that this question needed to be answered. This study, then, documents that children and adults were not found to be different in this regard.”
With advances in technology, it is not unrealistic that the integration of digital models and cone-beam computed tomography scans can provide skeletal arch analysis to determine ultimate arch form and size. Individualized arch forms are currently available through several vendors. OrthoCAD’s virtual setups permit customizing the arch form for each patient based on the pretreatment model. Ormco’s Insigna and SureSmile produce archwires customized for each patient.