Introduction
Previous studies have shown that most practitioners plan to maintain intercanine and intermolar widths during orthodontic treatment with fixed appliances. The aim of this study was to determine whether this was put into practice by clinicians during the latter stages of orthodontic treatment with fixed appliances.
Methods
This 2-part investigation was a laboratory-based measurement study at Bristol Dental Hospital, United Kingdom, from 2005 to 2007. Using standardized maxillary and mandibular study models with identical intermolar and intercanine widths but with differing degrees of tooth misalignment, 30 clinicians were asked to fabricate final working archwires according to their normal clinical practice. Then the intercanine and intermolar widths of the archwires were measured. In the second part of the study, the same intra-arch dimensions were measured directly from 50 pretreatment and posttreatment patient study models obtained from a subsample of 10 of the clinicians.
Results
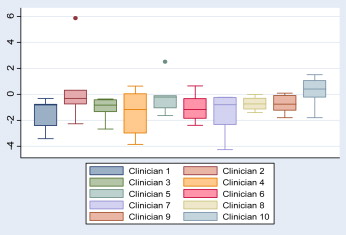
The intercanine and intermolar widths measured on the adapted archwires from the standardized study models showed wide variations in the results, even though the intercanine and intermolar widths of the models were identical. Data from 50 treated patients also showed that, in most, there were wide variations in intercanine and intermolar widths between the patients’ pretreatment and posttreatment study models.
Conclusions
Although most clinicians aim to maintain the pretreatment arch form, this study shows that this is often not transferred to clinical practice.
Editor’s comment
Are we hypocrites when it comes to fabricating the final working archwires for our patients? We claim to believe in maintaining the original arch form when planning treatment, but do we manage to follow through with that objective? Studies show that we can justify some expansion of the mandibular first molars by uprighting them during treatment. After all, this uprighting is known to be a normal change with maturation between the ages of 7 and 15 years. But routine expansion of intercanine width when correcting most malocclusions has proven to be a dangerous practice in the long term. Arch form has been in question since at least Angle’s time. He realized that changes in arch form were not stable and tended to relapse. This reality is not likely to change in the future. This study, conducted in the United Kingdom, points out the apparent inaccuracies of archwire formation, especially when fabricating final finishing arches, and the results are not surprising. Many clinicians use archwires right out of the box, picking wires that roughly conform to the canine and molar dimensions. The advent of the straight-wire appliance has discouraged many from placing bends, whether they are first, second, or third order.
You will want to read this entire article to fully understand the design of this clinical study. As a clinician, I would have loved to participate in the second part of this study, which required measuring posttreatment outcomes. I know I agree with 1 reviewer of this research who said, “This study serves as a reminder to all of us that orthodontists, not the orthodontic manufacturers, should determine arch form.” Although most clinicians aim to maintain pretreatment arch forms, this study shows that this goal was often not transferred to clinical practice.