Introduction
The aim of this study was to use low-dose coronal computed tomography (CT) scans to evaluate the treatment and postretention effects of rapid maxillary expansion (RME) on the maxillary central incisors, midpalatal suture, and nasal cavity.
Methods
Multi-slice coronal CT scans of 17 subjects (7 boys, 10 girls; mean age, 11.2 years) were taken before RME (T0), at the end of active expansion phase (T1), and after the retention period of 6 months (T2). Measurements were made on 3 coronal scans perpendicular to the occlusal plane and passing through anterior nasal spine (anterior scan), the midpoint between anterior nasal spine and posterior nasal spine (middle scan), and posterior nasal spine (posterior scan). Statistical analyses were performed with analysis of variance (ANOVA) for repeated measures with post-hoc tests.
Results
The transverse dimensions of the midpalatal suture and nasal cavity showed statistically significant T0 to T1 increments in all 3 coronal scans. The roots of the maxillary central incisors were more divergent than the crowns at both T1 and T2. All T0-to-T1 measurements at the sutural and nasal levels decreased from the anterior to the posterior measurements. Between T1 and T2, all measurements exhibited statistically significant decreases with the exception of nasal width on the middle scan.
Conclusions
When analyzed on coronal CT scans, the maxillary halves were separated by RME in a parallel manner and not in a triangular shape. At T2 after RME therapy, the suture appeared reorganized, and the expansion of the nasal cavity was stable.
Rapid maxillary expansion (RME) originated with Angell in 1860. This orthopedic treatment was reported and discussed frequently in the early dental, orthodontic, and rhinologic literature as both a potential nonextraction orthodontic technique and a method to improve nasal respiration. Many studies have investigated the maxillary response to RME in the sagittal and vertical dimensions as assessed on lateral cephalograms. Cephalometric studies on either posteroanterior (PA) headfilms or occlusal radiographs showed possible changes induced by RME in the transverse dimension. The use of PA cephalograms to quantify the amounts of expansion and concurrent dentoskeletal changes has some difficulties related to the reproducibility of head posture and the accuracy of landmark identification because of superimposition of different anatomic structures or poor radiographic techniques. In recent years, there has been growing interest in the use of tridimensional methods of investigation such as multislice computed tomography (CT) scans to evaluate the transverse effects of RME. Currently, there are few scientific investigations on coronal CT scans, although they would add valuable information to existing observations on axial CT scans of the palatal and nasal areas.
Garib et al compared the dentoskeletal effects produced by tooth-tissue–borne RME (4 girls, aged 11.4-13.6 years) and tooth-borne RME (4 girls, aged 11.5-13.9 years) with coronal CT scans after a 3-month retention period. The transverse increase at the level of the nasal floor corresponded to a third of the amount of screw activation (7 mm). Tooth-borne (hyrax) and tissue-borne (Haas type) expanders tended to produce similar orthopedic effects. This study did not assess the changes in the midpalatal suture on the coronal scans. Podesser et al investigated the transverse dimension of the maxilla including the nose, maxillary bones, and dental arches based on standardized coronal CT scans of 9 children with a mean age of 8.1 years. This group showed maxillary expansion and increasef nasal width (1.2 mm) accompanied by tipping of dentoalveolar structures. The postexpansion opening of the midpalatal suture on the coronal scans was evaluated at the canine and first molar levels on the palatal aspect of the suture (1.52 and 1.60 mm, respectively). No data were provided with regard to the nasal aspect of the midpalatal suture. On the other hand, conventional coronal tomograms showed recently that maxillary expansion can be accompanied by increases in the area and volume of the nasal cavity.
The aim of this investigation was to evaluate the treatment and postretention dentoskeletal effects of RME at the dental, maxillary, and nasal levels by using low-dose coronal CT scans.
Material and methods
Our study sample comprised 17 healthy white children (7 boys, 10 girls) with a mean age of 11.2 years (range, 8-14 years) who sought orthodontic treatment at the Department of Orthodontics of the dental school at the University of Rome “Tor Vergata” in Italy. The criteria for selection of the treatment group were as follows: constricted maxillary arches or unilateral or bilateral posterior crossbite, some crowding, and at least 1 maxillary canine having intraosseous displacement as assessed by panoramic radiographs. The exclusion criteria were age above 15 years, stage in cervical vertebral maturation as assessed on a lateral cephalogram more advanced than CS4 (postpubertal), no maxillary first molars, metallic restorations on the maxillary posterior teeth, periodontal diseases, previous orthodontic treatment, and genetic disease.
This project was approved by the ethical committee at the University of Rome, “Tor Vergata,” and informed consent was obtained from the parents. Each patient underwent a standardized protocol with RME in the form of the butterfly palatal expander similar to the basic design of Haas. A butterfly-shaped stainless steel framework was cemented through bands on the maxillary first molars and extended forward to the palatal surfaces of the deciduous molars. The expansion screw was activated 2 turns per day (0.25 mm per turn) for 14 days, thus reaching the total amount of expansion of 7 mm in all subjects. Then the screw was tied off with a ligature wire, and the butterfly palatal expander was kept on the teeth as a passive retainer for 6 months. This period of retention allowed for reorganization and reossification of the midpalatal suture after expansion.
Multislice coronal CT scans were taken before RME (T0), at the end of the active expansion phase (T1), and after the retention period of 6 months when the expander was removed (T2). The scans were carried out by a trained radiographer on the same scanner console primarily to evaluate the exact position of displaced intraosseous canines in the maxilla. All examinations were performed in the Department of Radiology, University of Rome “Tor Vergata” on a CT scanner with a Dentascan reconstruction program (Light-Speed 16, General Electric Medical Systems, Milwaukee, Wis) used to study the maxillofacial region. This machine is equipped with 16 detector rows and has a minimum rotation time of 0.5 seconds, and collimation between 0.75 and 1.5 mm with dose calibration. Subsequent scans were taken with 1.25-mm slice thickness, 0.6-mm interval, 11.25-mm table speed or rotation, 100 mA, 13.7-cm field of view, 512 × 512 matrix, and 0° gantry angle, with a low-dose protocol with 80 kV instead of the standard CT setting of 120 kV.
Each patient was positioned horizontally on the scanner table with the Camper’s plane perpendicular to the ground. The perpendicular light beams of the machine were used to standardize the head position in the 3 planes, thus allowing comparison of the images achieved before, during, and after expansion. During the CT scanning, the patients bit on a piece of gauze to keep the maxillary and mandibular teeth separated, and to avoid overlapping of dentofacial structures.
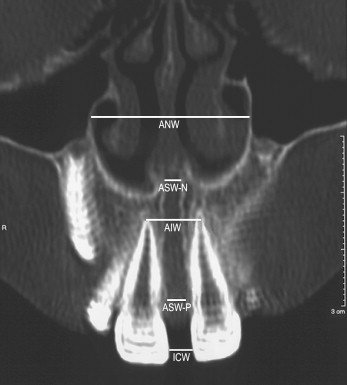
On the scanned images, measurements were made at the central incisors, midpalatal suture, and nasal cavity by using 3 coronal scans: perpendicular to the occlusal plane and passing through anterior nasal spine (ANS), the midpoint between ANS and posterior nasal spine (PNS), and PNS, respectively.
The anterior scan ( Fig. 1 ) included (1) interincisor crown width (ICW), the shortest transverse distance between the mesial surfaces of the crowns of the maxillary central incisors; (2) interincisor apex width (IAW), the transverse distance between the root apices of the maxillary central incisors; (3) anterior sutural width-palatal (ASW-P), the shortest transverse distance at the level of the alveolar bone crest level adjacent to the mesial surfaces of the roots of the maxillary central incisors, thus indicating the width of the anterior portion of the midpalatal suture on the palatal side; (4) anterior sutural width-nasal (ASW-N), the shortest transverse distance between the mesial contour of each maxillary half at the level of ANS, thus indicating the width of the midpalatal suture on the nasal side; and (5) anterior nasal width (ANW), the transverse width between the most lateral point of each nasal cavity.
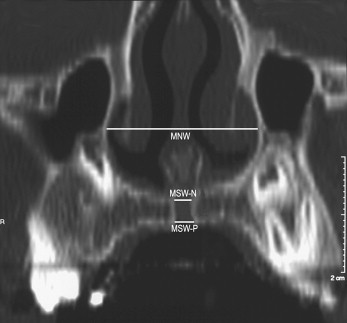
The middle scan ( Fig. 2 ) included (1) middle sutural width-palatal (MSW-P), the shortest transverse distance between the mesial contour of each maxillary half at the level of the palatal vault in the middle point between ANS and PNS, thus indicating the width of the middle portion of the midpalatal suture on the palatal side; (2) middle sutural width-nasal (MSW-N), the shortest transverse distance between the mesial contour of each maxillary half at the level of the nasal floor in the middle point between ANS and PNS, thus indicating the width of the middle portion of the midpalatal suture on the nasal side; and (3) middle nasal width (MNW), the transverse width between the most lateral point of each nasal cavity.
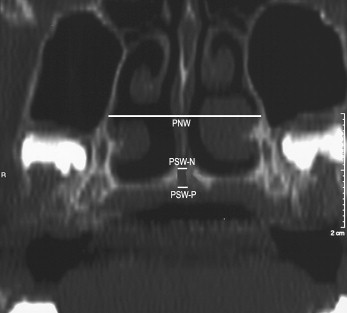
The posterior scan ( Fig. 3 ) included (1) posterior sutural width-palatal (PSW-P), the shortest transverse distance between the mesial contour of each maxillary half at the level of the palatal vault in correspondence of PNS, thus indicating the width of the posterior portion of the midpalatal suture on the palatal side; (2) posterior sutural width-nasal (PSW-N), the shortest transverse distance between the mesial contour of each maxillary half at the level of the nasal floor in correspondence of PNS, thus indicating the width of the posterior portion of the midpalatal suture on the nasal side; and (3) posterior nasal width (PNW), the transverse width between the most lateral point of each nasal cavity.
Statistical analysis
All measurements were made by 2 operators (F.B. and R.L.) at the same scanner console, and they were repeated a month later at the same console by 1 operator (F.B.). Systematic and random errors were calculated by comparing the first and the second measurements with paired t tests and Dahlberg’s formula, respectively. No statistically significant differences ( P >0.05) were found between the first and second measurements for any of the analyzed variables; the range for random errors was 0.01 to 0.18 mm. The correlation between the first and second readings was calculated by using the Spearman correlation analysis and represented with the r value. All measurement error coefficients were found to be close to 1.00 and within acceptable limits (range, 0.89-0.99). The mean differences in measurements at T0, T1, and T2 were contrasted by means of the Friedman analysis of variance (ANOVA) for repeated measures followed by the Tukey post-hoc test (SigmaStat version 3.5, Systat Software, Point Richmond, Calif). The level of significance was P <0.05, and the power of the study exceeded 0.80.
Results
In the evaluation of the changes between T0 and T1 ( Table ), all measurements showed statistically significant increments. ICW and IAW increased by 2.54 and 3.49 mm, respectively. The midpalatal suture was opened in all subjects, and it showed statistically significant increments at all 3 coronal scans. All T0-to-T1 increases at the sutural and nasal levels decreased from the anterior to the posterior measurements.
| T0 | T1 | T2 | Comparison of the means | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Measurement (mm) | Mean | SD | Mean | SD | Mean | SD | T0 vs T1 | T1 vs T2 | T0 vs T2 |
| ICW | 0.48 | 0.58 | 3.02 | 0.87 | 0.57 | 0.59 | 2.54 ∗ | −2.45 ∗ | 0.09 NS |
| IAW | 6.55 | 1.21 | 10.04 | 1.04 | 8.53 | 1.56 | 3.49 ∗ | −1.51 ∗ | 1.98 ∗ |
| ASW-P | 0.26 | 0.25 | 2.68 | 0.62 | 0.28 | 0.22 | 2.42 ∗ | −2.40 ∗ | 0.02 NS |
| MSW-P | 0.29 | 0.20 | 2.10 | 0.74 | 0.35 | 0.22 | 1.81 ∗ | −1.75 ∗ | 0.06 NS |
| PSW-P | 0.24 | 0.17 | 1.08 | 0.34 | 0.24 | 0.24 | 0.84 ∗ | −0.84 ∗ | 0.00 NS |
| ASW-N | 0.24 | 0.22 | 2.66 | 0.62 | 0.27 | 0.21 | 2.42 ∗ | −2.39 ∗ | 0.03 NS |
| MSW-N | 0.23 | 0.17 | 2.15 | 0.69 | 0.30 | 0.22 | 1.92 ∗ | −1.85 ∗ | 0.07 NS |
| PSW-N | 0.21 | 0.18 | 1.13 | 0.52 | 0.24 | 0.24 | 0.92 ∗ | −0.89 ∗ | 0.03 NS |
| ANW | 19.57 | 1.68 | 21.12 | 1.47 | 20.69 | 1.53 | 1.55 ∗ | −0.43 ∗ | 1.12 ∗ |
| MNW | 26.01 | 2.18 | 27.41 | 2.21 | 27.17 | 2.32 | 1.40 ∗ | −0.24 NS | 1.16 ∗ |
| PNW | 24.39 | 1.80 | 25.4 | 1.77 | 24.98 | 1.90 | 1.01 ∗ | −0.42 ∗ | 0.59 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


