Introduction
The aim of this study was to describe a natural and anatomic lingual arch form obtained from subjects with normal occlusion that could be used, with other criteria, in the construction of personalized setups for the lingual straight-wire technique.
Methods
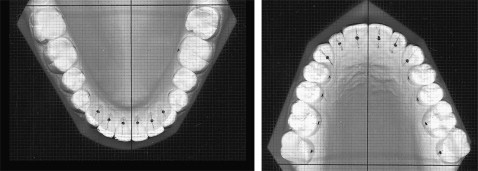
The study sample comprised 58 pairs of dental casts of the arches of 58 southern Europeans (37 women, 21 men) with ideal natural occlusions. After the reference points of the dental arches were identified and marked, the dental casts were scanned. The exact position of the models on the scanner was established by using an acetate sheet with a Cartesian reference system. For each image, 14 reference points (x, y) were measured and recorded. The measurements were processed with software to select the polynomial function that best described the shape of the dental arches. The ninth-degree polynomial function was selected to represent the lingual arch form of both arches. Distribution analysis of the x and y values of each tooth in each arch resulted in the creation of 3 groups (small, medium, and large) to verify the most appropriate measures of the central tendencies of our data.
Results
Statistical analysis showed no significant sex difference in the medians of the 6 parameters used to measure depth and width in both arches. A representation of the variability of the lingual curve of our sample was created to document at least 3 sizes of the representative curve of the central tendency for our data. No statistically significant differences in shape were found between men and women, considering the medians as a measure of the central tendencies.
Conclusions
Three lingual curves (small, medium, and large) for the maxillary and mandibular arches, representing the mean values of our sample, were developed and can be used as guides for the setup in the lingual straight-wire technique.
Editor’s comment
When it comes to arch forms, I still remember the day I viewed my first maxillary lingual archwire. Calling it a “mushroom” arch did little to calm my fears of ever trusting it to align teeth properly. I will admit to learning much about bending wires while treating those first 10 patients whom I started with a lingual appliance. With this experience in my background, I can appreciate how someone in a residency is eager to make sense out of the archwires needed to use with any lingual appliance.
Although clinicians understand the need to individualize each patient’s archwire to fit his or her needs in treatment, there are recognized complications to this practice. We know how labial arch forms vary with differing groups of patients, not to mention archwires made with superelastic properties. These researchers believed it logical to base their ideal lingual arch forms on subjects with normal occlusion selected on the basis of geometric similarity, ethnicity, and type of malocclusion. Their sample comprised 58 pairs of dental casts of the arches of white subjects of southern European ancestry (mainly Italian and Spanish origins). Reference points for calculation of the shape of each arch were identified and marked on the lingual surface of each tooth (from the left second molar to the right second molar) of each dental cast by 1 operator. The purpose of this study was to analyze the lingual shape of the maxillary and mandibular dental arches in a sample of adults for constructing personalized setups for the lingual straight-wire technique.
A distributive analysis of the x and y values for each tooth was performed to determine the measure of central tendency most appropriate for the data. Another reason of the research was to identify 3 curves, corresponding to the 3 groups (small, medium, and large), which could interpolate the measures of central tendency to represent the sample with the highest level of accuracy. It is hoped that the coordination of these maxillary and mandibular curves will enable these arch forms to be used as guides in the design of a lingual straight-wire technique.