Armamentarium
|
History of the Procedure
Closely related to the principles of post-traumatic osseous repair, the development of distraction osteogenesis (DO) received an outstanding contribution from the work of Ilizarov. The Russian surgeon developed innovative devices for skeletal fixation and osteotomy techniques that deliver minimum trauma to the periosteum and to the bone marrow. His landmark set of clinical experiments led to the discovery of the biologic basis of osteodistraction, the Ilizarov effects, which suggest that gradual traction applied on living tissues can stimulate and maintain regeneration and active growth and that the mass and shape of bones and articulations depend on their blood supply and their functional burden. His studies later determined the technical protocols for DO and are still used as a basic reference for studies in this field.
Applications in craniofacial surgery were first seen in 1973, when Snyder et al. applied the approach to mandibular lengthening in a canine animal model. Almost 20 years passed before McCarthy et al., in 1992, published the first report of mandibular lengthening in children with congenital mandibular deficiency. Thereafter, the role of DO rapidly expanded to the midface and to nearly all classic approaches to craniofacial reconstruction. In humans, DO has been used for surgical palatal expansion, mandibular symphysis elongation, correction of congenital facial abnormalities, treatment of cleft conditions, repair of continuity defects of the mandible, alveolar crest augmentation, and mandible reconstruction after tumor resection.
Since the first case report on alveolar DO in the literature, presented by Chin and Toth, numerous case series and clinical investigations, in addition to two prospective clinical studies, have been published.
History of the Procedure
Closely related to the principles of post-traumatic osseous repair, the development of distraction osteogenesis (DO) received an outstanding contribution from the work of Ilizarov. The Russian surgeon developed innovative devices for skeletal fixation and osteotomy techniques that deliver minimum trauma to the periosteum and to the bone marrow. His landmark set of clinical experiments led to the discovery of the biologic basis of osteodistraction, the Ilizarov effects, which suggest that gradual traction applied on living tissues can stimulate and maintain regeneration and active growth and that the mass and shape of bones and articulations depend on their blood supply and their functional burden. His studies later determined the technical protocols for DO and are still used as a basic reference for studies in this field.
Applications in craniofacial surgery were first seen in 1973, when Snyder et al. applied the approach to mandibular lengthening in a canine animal model. Almost 20 years passed before McCarthy et al., in 1992, published the first report of mandibular lengthening in children with congenital mandibular deficiency. Thereafter, the role of DO rapidly expanded to the midface and to nearly all classic approaches to craniofacial reconstruction. In humans, DO has been used for surgical palatal expansion, mandibular symphysis elongation, correction of congenital facial abnormalities, treatment of cleft conditions, repair of continuity defects of the mandible, alveolar crest augmentation, and mandible reconstruction after tumor resection.
Since the first case report on alveolar DO in the literature, presented by Chin and Toth, numerous case series and clinical investigations, in addition to two prospective clinical studies, have been published.
Indications for the Use of the Procedure
After dental extractions, a rapid process of buccal plate resorption occurs. As result of this, very often the oral and maxillofacial surgeon encounters a ridge that has sufficient crestal bone height but is too narrow for implant insertion. In addition to augmentation by alveolar ridge split, onlay block, or guided bone regeneration (GBR), distraction osteogenesis can be used to gain width for the alveolus. The advantage of this technique is distraction histogenesis of associated soft tissues, which provides sufficient keratinized tissue coverage of the increased volume of the expanded crest.
Resorption of the alveolar crest takes place in all dimensions yet can generally be thought of as bidimensional—vertical and horizontal. In general, vertical bone loss seldom occurs strictly without considerable loss of bone in the horizontal dimension, with a resultant shift of alveolar bone mass to the lingual. Frequently, for both the maxilla and the mandible, a loss of buccal bone mass occurs initially, including the buccal crest. With further resorption, the lingual crest is lost and alveolar vertical bone loss develops. When vertical loss is 5 mm or more, vertical distraction is indicated. However, because of vector control problems, vertical distraction of a typical alveolar segment further shifts the alveolar bone mass lingually. Therefore, unidirectional distraction may improve crestal height, but it compromises alveolar position, preventing ideal implant placement. During the course of distraction, traction from the lingual/palatal periosteum, muscles, and attached gingiva prevents maintenance of an axial vector. One solution to this technical problem is to use a bidirectional device that moves the segment both vertically and buccally.
The use of small, low-profile devices, which can be used without substantially interfering with the occlusal and esthetic functional requirements, enables the surgeon to manipulate small segments of osteotomized bone into more ideal positions for dental implant installation. A bidirectional device, the bidimensional crest distracter (2DCD; Surgi-Tec, Bruges, Belgium), was designed to enable both vertical and horizontal distraction. The device works in sequence, first by vertical distraction and then by horizontal distraction, to correct horizontal deflection.
Limitations and Contraindications
Although both total edentulous maxillary distraction and full mandibular horseshoe alveolar distraction have been used to gain vertical height, these procedures have largely been supplanted by local osteotomies done either in the posterior or anterior part of the mouth to avoid major surgery.
The surgeon must understand that alveolar form in the ablated condition is never ideal; after distraction osteogenesis, the alveolar process needs further reconstruction with bone graft material to be made suitable for dental implants. Most often, bone grafting can be done at the same time as implant placement; however, in some cases the distraction is done in preparation of the soft tissue envelope for a definitive grafting procedure.
Once used extensively, alveolar distraction has declined in popularity with the development of osteoperiosteal flap procedures, particularly the alveolar split (book bone flap) and the sandwich osteotomy interpositional graft procedure. The use of bone morphogenetic protein-2 (BMP-2) has increased the capability of both fixed osteoperiosteal flaps and those using bone transport achieved by distraction osteogenesis.
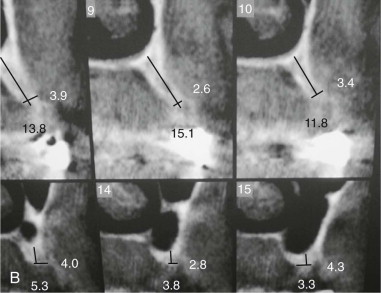
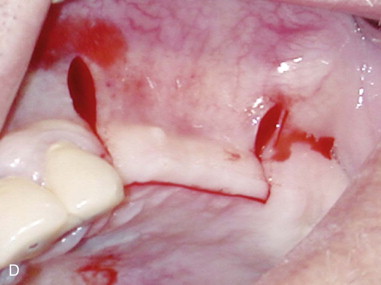
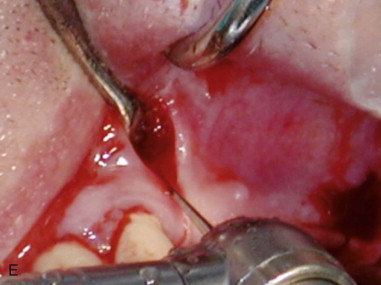
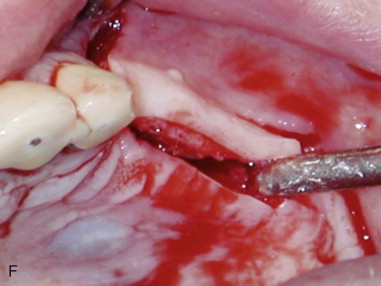
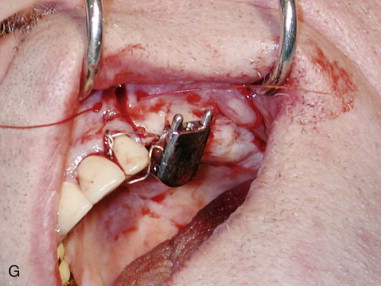
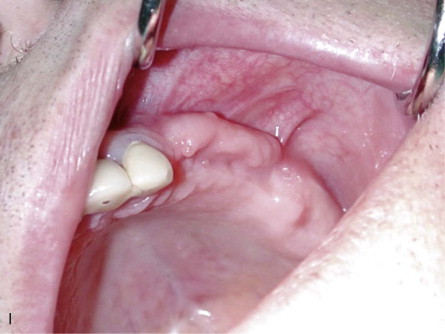
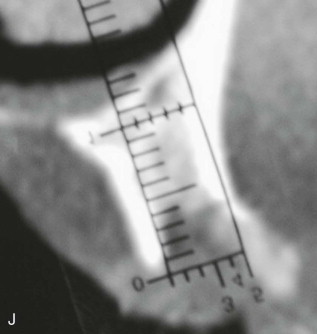
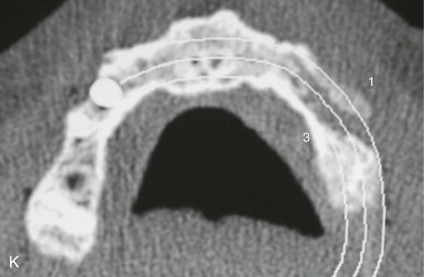
Technique: Alveolar Width Distraction
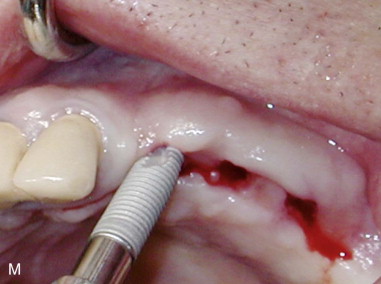
A 67-year-old male is referred for bone augmentation of the upper left maxilla. Examination of a computed tomography (CT) scan reveals a residual ridge 2.6 mm wide. A horizontal distraction device, or crest widener (e.g., Laster Crest Widener; M.I.S, Shlomi, Israel), is used to expand the alveolar crest. The crest widener consists of four associated arms, each couplet moving apart to separate the bone when activated. The advantage of the crest widener is that the periosteum is not stripped; thus, the blood supply to the distracted segment is not impaired ( Figure 21-1, A to C ).





Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


