Armamentarium
A—Vestibuloplasty Procedure
|
B—Skin Graft Procurement
|
C—Skin Graft Preparation/Application
|
History of the Procedure
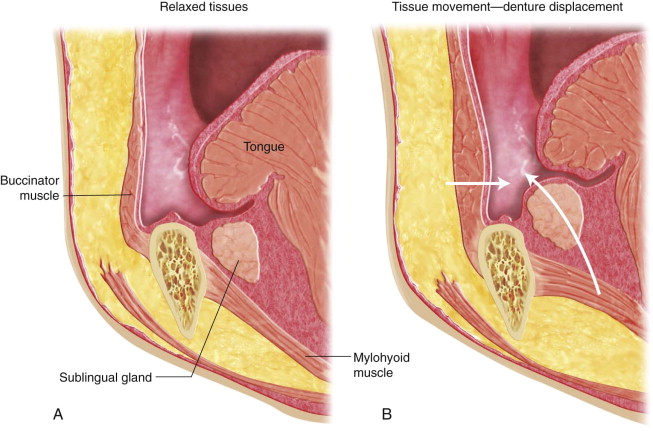
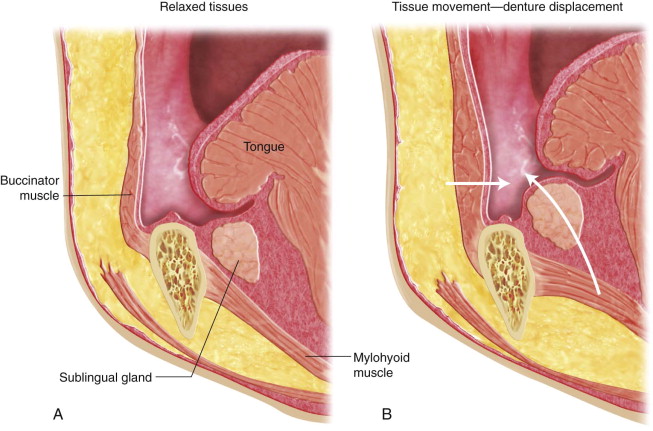
The use of skin grafts to create a buccal vestibule in patients who present with inadequate soft tissue drape to support a denture base dates back to 1915 when Thiersch grafts were placed over the mandible via percutaneous pockets later opened to expose the underlying skin graft providing a new sulcus. Weiser was probably the first to apply skin pouches perorally to the buccal vestibule. Pickrell, Kilner and Jackson, and Kazangian all added publications to the literature on the evolving vestibuloplasty technique. A publication by Pichler and Trauner in 1930 delineated many of the principles of this procedure (need for dissection close to the periosteum, hip skin donor site, allowing donor site to crust) that hold true to the present day. The lowering of the genioglossus muscles, the mylohyoid muscles from the cuspid region posteriorly, and of the mental foramen added more versatility to the vestibuloplasty. Schuchardt reported on the skin grafting of the labiobuccal surface of the mandible in 1952. In 1959 the technique of submucous vestibuloplasty in the maxilla was described by Obwegeser to extend fixed tissue on the alveolar ridge. This procedure was found to be particularly useful in patients who showed alveolar resorption with resulting encroachment of the muscle attachments on the crest of the ridge. In 1963 Obwegeser presented total floor of the mouth lowering by sectioning the mylohyoid as far forward as possible and sectioning parts of the genioglossus, which greatly enhanced the popularity of the vestibuloplasty. Although the evolution of implants has made the vestibuloplasty procedure uncommon for increasing denture surface area, other pertinent indications remain for the technique, and it should continue to be part of the training of oral and maxillofacial surgeons. The typical atrophic mandibular ridge has a small line of attached mucosa at the crest of the ridge, whereas all of the remaining mucosa of the denture-bearing area can be elevated by the movement of the lips, cheeks, and tongue displacing a denture ( Figure 18-1 ). VSG and LFM procedures result in a nondisplaceable tissue over the entire denture base. The graft’s firm attachment to the periosteum ridge allows for denture stability even in cases where no significant ridge height can be created by the procedures. An additional advantage offered by VSG and LFM surgery is that skin utilized in the grafts tends to react to pressure with a hyperkeratotic response, whereas mucosa tends to ulcerate under similar stress. Skin seems to be a more comfortable surface to the patient than is mucosa. There are indications from the literature, such as a study by Landesman and colleagues, that not only do VSG and LFM procedures not cause increased mandibular bone resorption, but they may actually diminish the rate of resorption.
History of the Procedure
The use of skin grafts to create a buccal vestibule in patients who present with inadequate soft tissue drape to support a denture base dates back to 1915 when Thiersch grafts were placed over the mandible via percutaneous pockets later opened to expose the underlying skin graft providing a new sulcus. Weiser was probably the first to apply skin pouches perorally to the buccal vestibule. Pickrell, Kilner and Jackson, and Kazangian all added publications to the literature on the evolving vestibuloplasty technique. A publication by Pichler and Trauner in 1930 delineated many of the principles of this procedure (need for dissection close to the periosteum, hip skin donor site, allowing donor site to crust) that hold true to the present day. The lowering of the genioglossus muscles, the mylohyoid muscles from the cuspid region posteriorly, and of the mental foramen added more versatility to the vestibuloplasty. Schuchardt reported on the skin grafting of the labiobuccal surface of the mandible in 1952. In 1959 the technique of submucous vestibuloplasty in the maxilla was described by Obwegeser to extend fixed tissue on the alveolar ridge. This procedure was found to be particularly useful in patients who showed alveolar resorption with resulting encroachment of the muscle attachments on the crest of the ridge. In 1963 Obwegeser presented total floor of the mouth lowering by sectioning the mylohyoid as far forward as possible and sectioning parts of the genioglossus, which greatly enhanced the popularity of the vestibuloplasty. Although the evolution of implants has made the vestibuloplasty procedure uncommon for increasing denture surface area, other pertinent indications remain for the technique, and it should continue to be part of the training of oral and maxillofacial surgeons. The typical atrophic mandibular ridge has a small line of attached mucosa at the crest of the ridge, whereas all of the remaining mucosa of the denture-bearing area can be elevated by the movement of the lips, cheeks, and tongue displacing a denture ( Figure 18-1 ). VSG and LFM procedures result in a nondisplaceable tissue over the entire denture base. The graft’s firm attachment to the periosteum ridge allows for denture stability even in cases where no significant ridge height can be created by the procedures. An additional advantage offered by VSG and LFM surgery is that skin utilized in the grafts tends to react to pressure with a hyperkeratotic response, whereas mucosa tends to ulcerate under similar stress. Skin seems to be a more comfortable surface to the patient than is mucosa. There are indications from the literature, such as a study by Landesman and colleagues, that not only do VSG and LFM procedures not cause increased mandibular bone resorption, but they may actually diminish the rate of resorption.
Indications for the Use of the Procedure
The main current indications for vestibuloplasty can be divided into four categories for the present discussion:
- 1.
Ridge extension and lowering or otherwise altering the prosthesis displacing submucous attachments to allow for better denture fit is the original indication for vestibuloplasty procedures in their many manifestations in the maxilla and mandible.
- 2.
Procedures that attempt to reconstruct edentulous bone loss by various means frequently require vestibuloplasty procedures to complement and complete the osseous reconstruction. The compromised soft tissue drape resulting after such osseous augmentations can be markedly improved with soft tissue vestibuloplasties.
- 3.
Inadequate or inappropriate soft tissue drape in cases where resection with or without grafting has been previously performed and prosthetic restoration demands improvement of the soft tissue drape.
- 4.
Occasionally implants are placed so that they emerge in nonattached mucosa, and there are those who feel that the success of restorations based on these implants can be markedly improved with the creation of an attached mucosa/implant interface. The stability of the peri-implant mucosa is important for the overall stability of the dental implant and the maintenance of bone health around an implant. Whether the stability is secured by nonkeratinized mucosa or keratinized attached mucosa is a point of discussion. Some investigators report no difference in the maintenance of peri-implant bone levels, whereas others report an increased risk for peri-implant bone loss when the implant is surrounded by alveolar mucosa. Insufficient keratinized mucosa in the vicinity of implants does not necessarily mediate adverse effects on hygiene management.
Limitations and Contraindications
The general health of the patient must be considered as a limiting factor in vestibuloplasty, as these procedures frequently require a 2- to 3-hour or so general anesthetic for completion. Patients who have been irradiated in the head and neck require extra precaution in all surgical procedures in the field of treatment. In mandibular vestibuloplasties, temporary or permanent mental nerve paresthesias are common, and the patient must understand this possibility prior to surgery and be able to tolerate these deficits. Donor and operative site pain can be significant, and those who feel they would do poorly with such a degree of postoperative pain should be excluded from these surgeries. Donor site color and texture will be altered, and this may dissuade some from the VSG procedure for cosmetic considerations. Mandibular ridges of less than 15 mm of body height are less likely to result in adequate vestibular depth after VSG and LFM; however, a broader immobile graft area after such procedures may improve denture-wearing ability even in the face of decreased mandibular bone height. Maxillary myotomies and grafts can be performed by open or closed techniques, and although 10 to 15 mm of ridge height and some palatal depth allow for more successful augmentations, the facial aspect of the maxilla allows for relocation of the muscle attachments more extensively without fear of muscle detachment complications than is possible in the mandible. Around the midline of the mandible, dissection in the supraperiosteal plane should end about 1 cm above the inferior border of the mandible to prevent mentalis detachment and resultant drooping of the chin. Sharp mylohyoid ridge undercuts may be removed if excessive, but atrophy will occur after detachment of the mylohyoid in the LFM procedure. Sharpness of the genial tubercles will also atrophy after the genioglossus attachments are removed superiorly, but recontouring may be required if genial tubercles are large. Any recontouring procedures required should be done prior to VSG and LFM because it requires subperiosteal dissection. Healing of 2 to 3 months should be allowed prior to skin grafting over the area of excised bone. Although skin grafts can be sutured in place, surgical stents allow for accurate adaptation to the labial-buccal and lingual areas. Most consider the surgical stent to be an important component of VSG and LFM procedures, and laboratory capabilities must exist for those who contemplate such preprosthetic surgeries.
Technique: Graft Donor Sites
Because several vestibuloplasty techniques require a skin or mucosal graft, the technique for both of these procedures will be outlined prior to a discussion of techniques for vestibuloplasty. For obtaining a split-thickness skin graft, please refer to the reconstruction chapter of this text. If the determination is made to utilize a mucosal graft, it can be obtained from the palate or buccal mucosa. In the case of the palate, the graft is excised in a horseshoe shape in a supraperiosteal plane, whereas in the buccal mucosa a spindle-shaped graft is excised without muscle and as superficial to the lamina propria as possible. The palatal site is left to granulate in and may or may not be covered with a protective stent. The buccal mucosa graft site is closed with resorbable sutures in a superficial plane to prevent entrapment of muscle tissues in the scar, thereby minimizing the chance of trismus after healing. A study by Hashemi and colleagues suggested that Alloderm (Lifecell Corporation, Bridgewater, New Jersey) is a suitable alternative to mucosal and skin grafts in vestibuloplasty procedures. Alloderm is donated human skin that is aseptically processed to remove all cells, maintaining only a skin matrix framework. Collagen and elastic fiber make up this U.S. Food and Drug Administration (FDA)—approved human tissue allograft, which has been in use since the early 1990s in burn injury treatment as well as in plastic and periodontal surgery. Although Alloderm overcomes many of the problems associated with mucosal and skin grafts, including donor site morbidity, it is associated with increased financial considerations.
Technique: Stents
All grafts are sutured inferiorly and superiorly to the vestibuloplasty site and held in place with a previously prepared surgical splint. Alternatively, grafts can be adapted closely to the undersurface of the stent and secured to it with Dermabond (Ethicon, Somerville, New Jersey). The stent is designed on a study model, and the borders of the stent are perforated so the green modeling compound can be heated and applied for border molding after the myotomy is completed. The molded stent is attached to the mandible or maxilla with circummandibular wires or screws.
Technique: Vestibular Skin Grafting and Lowering of Floor of Mouth
Step 1:
Initial Incision and Dissection
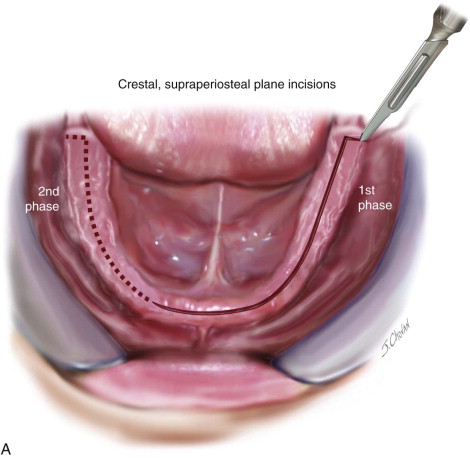
A crestal incision is made with a #15 blade running from retromolar pad to retromolar pad at the junction of the free and attached gingiva in a supraperiosteal plane. As the supraperiosteal dissection proceeds, it is important to remove all of the soft tissue from the periosteum and displace it inferiorly. Failure to remove any soft tissue will result in graft mobility where it remains. Small periosteal perforations may occur but will not be as unfavorable as leaving soft tissue attached as long as they are less than 1 sq cm in size. When a margin of mucosa is identified, double-ended skin hooks are applied and light tension is utilized to assist in the dissection from the periosteum with the front or back of the #15 blade, a periosteal elevator, or a peanut. As the mental neurovascular bundle is approached, it is easily identified and left in the subperiosteal plane, and shallow dissection here avoids damage to this structure. Patient education should always include the possibility of mental nerve paresthesia/anesthesia. The posterior limit of the dissection should be at the external oblique line, whereas the anterior limit in the midline should not exceed 1 cm from the inferior border of the mandible to prevent sagging of the chin ( Figure 18-2, A ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


