The retromolar fossa is an anatomically suitable skeletal anchorage site. The aim of this report was to introduce a novel appliance for the correction of skeletal Class III malocclusions with mandibular dentition distalization. The placement site and the procedure of the ramal plate are described. The resulting force vectors are parallel to the functional occlusal plane leading to efficient molar distalization. This approach is demonstrated with 2 adult patients who refused a surgical treatment option. This ramal plate may be indicated for total arch distalization for nonextraction and nonsurgical cases.
Highlights
- •
A ramal plate was placed in the retromolar fossa to distalize the mandibular dentition.
- •
Procedures and placement site of the ramal plate are described in this report.
- •
Force vectors and the implemented mechanics are described.
- •
A ramal plate can provide arch distalization for nonextraction, nonsurgical patients.
A severe anteroposterior skeletal discrepancy in a patient with a Class III malocclusion is generally treated with orthognathic surgery. However, a mild to moderate skeletal Class III malocclusion can be treated by either surgery or camouflage. Traditionally, patients who were reluctant to undergo surgical procedures to improve their Class III dental relationships turned to camouflage orthodontic treatment with different extraction patterns according to the proclination of the mandibular incisors and the amount of negative overjet.
Recently, temporary skeletal anchorage devices (TSADs) have decreased the need for extractions and surgical procedures. Previous studies have reported the achievement of 4 to 5 mm of mandibular molar distalization using miniscrews in the retromolar area. Distalization of the mandibular molars enables retraction of the incisors to achieve a positive overjet. Other studies have reported successful mandibular total arch distalization using stainless steel miniscrews placed in the buccal shelf.
Miniplates can withstand the higher forces required to distalize the whole dentition, unlike miniscrews. Sugawara et al reported the use of miniplates for mandibular distalization, and they placed the miniplates on the mandibular body. In contrast, our ramal plates are installed medial to the anterior border of the ramus because the force vector might be more favorable from the retromolar area for some patients because it is more parallel to the functional occlusal plane.
Therefore, the purpose of this article is to introduce placement of a ramal plate in the retromolar fossa as a novel approach to efficient mandibular total arch distalization.
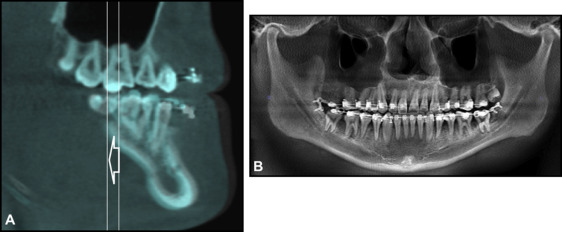
A ramal plate is placed in the retromolar fossa, located between the anterior border of the mandibular ramus and the temporal crest ( Fig 1 ). After doing the flap in the retromolar area, the L-plate (LeForte System; Jeil Medical, Seoul, Korea; length of the short arm, 10 mm; length of the long arm, 15.5 or 22 mm; diameter, 2.5 mm) is adapted to fit the bone surface. The third molars are extracted during the procedure. The anterior hole of the plate that extends into the oral cavity is positioned horizontally to be 3 mm lateral to the buccal surface of the second molar, and between the buccal groove of the second molar and its distal surface, anteroposteriorly ( Fig 2 ).
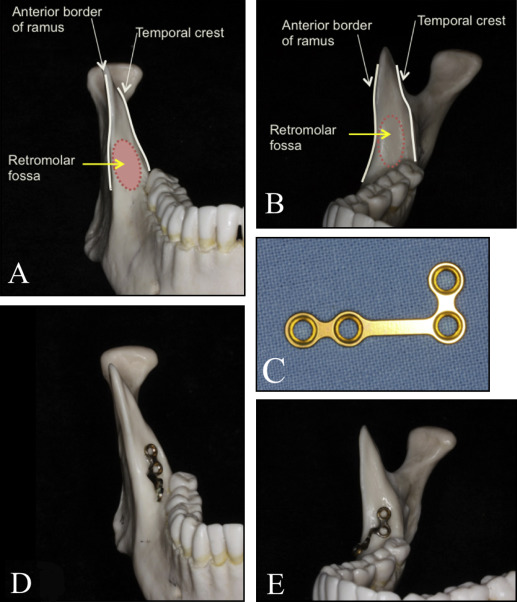
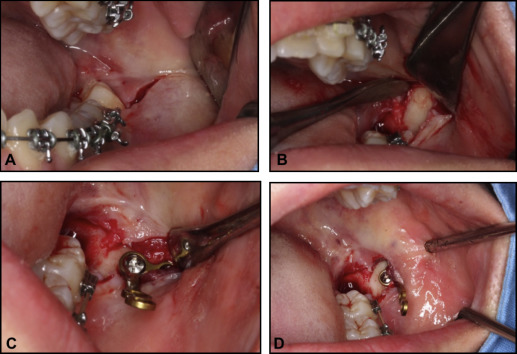
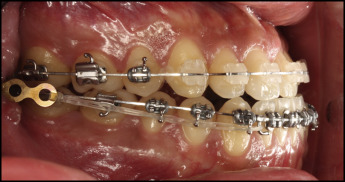
The plates are fixated with 2 screws (with pilot drilling), 2 mm in diameter, 5 mm in length. The flap is sutured (usually 2 sutures) over the plate, and the hook is extended out of the mucosa, vertically at the level of the second molar tube and horizontally within 3 to 6 mm lateral to the buccal surface of the second molar. Elastic chain can be tied around the anterior screw hole of the plate, or it might be cut occlusally to convert it into a hook for easier placement of elastics or nickel-titanium closed-coil springs that are connected to hooks crimped to the archwire between the lateral incisors and the canines immediately after the plate is placed ( Fig 3 ). Analgesics might be prescribed after placement to alleviate any postoperative pain.
Patient 1
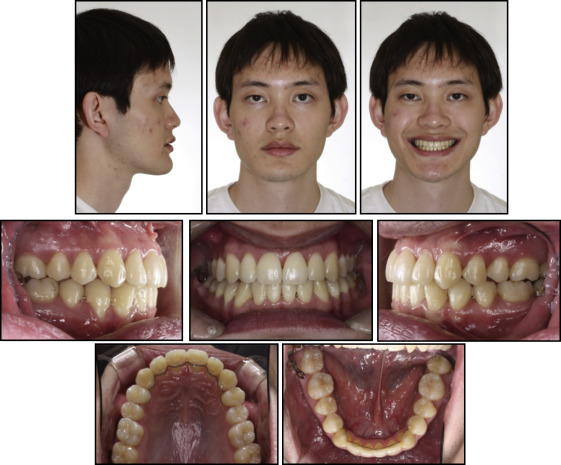
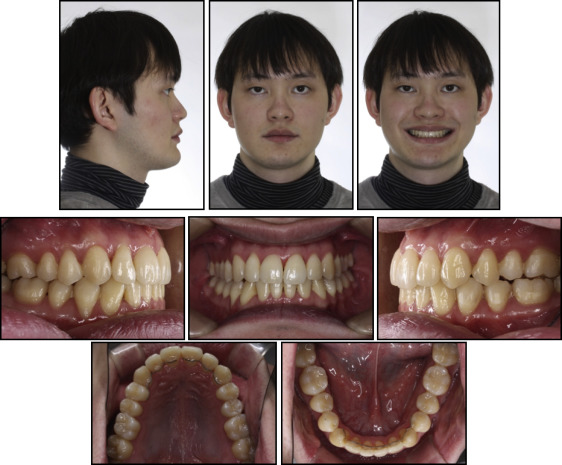
A 21-year-old man came with a chief complaint of “I cannot chew properly.” He had a brachyfacial, symmetrical face and a prognathic mandible with a Class III appearance.
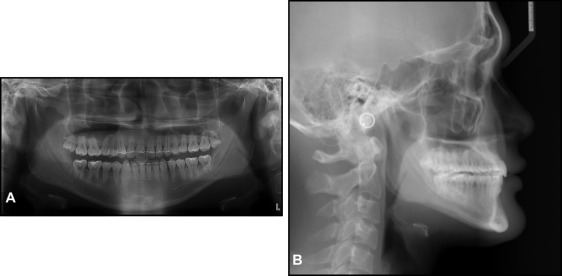
Intraorally, his maxillary central incisors showed an overjet of 1 mm and an overbite of 0.5 mm. He also had an anterior crossbite on his maxillary right lateral incisor and posterior open bites with a frontal and lateral tongue-thrust habit when swallowing. He had full-step Class III molar relationships on the right side and end-on Class III relationships on the left side with moderate crowding in both arches. He also had a 3-mm curve of Spee on the mandibular arch. The intermolar widths were narrow, and the mandibular posterior teeth were tilted lingually ( Fig 4 ). The mandibular right third molar was missing ( Fig 5 ).

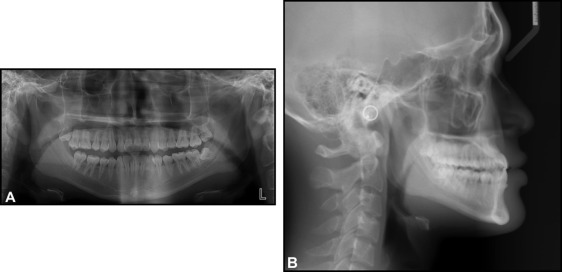
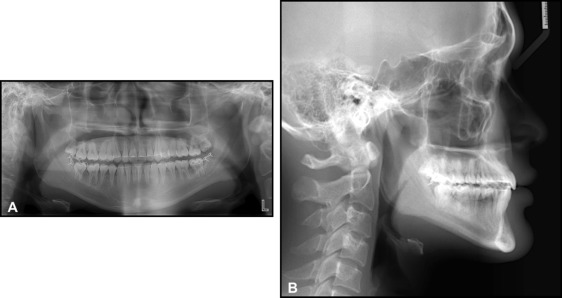
The patient had a skeletal Class III (ANB, −4.0°; Wits appraisal, −7.0 mm; Harvold analysis, 35.5 mm) with a hypodivergent growth pattern (FMA, 20.0°). The mandibular incisors were retroclined (IMPA, 79.0°), and the maxillary incisors were proclined (U1-FH, 127.0°). The interincisal angle was 134.5°, showing dental compensation of the skeletal Class III discrepancy ( Table I ).
| Measurement | Norm | Pretreatment | Posttreatment |
|---|---|---|---|
| Horizontal skeletal pattern | |||
| SNA (°) | 82.0 | 87.0 | 87.0 |
| SNB (°) | 80.0 | 91.0 | 89.5 |
| ANB (°) | 2.0 | −4.0 | −2.5 |
| A-point to N perpendicular (mm) | 1.1 | 0.5 | 1.0 |
| Pog to N perpendicular (mm) | −0.3 | 11.0 | 9.5 |
| Wits appraisal (mm) | −2.2 | −7.0 | −2.0 |
| Harvold analysis (mm) | 35.8 | 35.5 | 36.0 |
| Vertical skeletal pattern | |||
| Facial height ratio (posteroanterior) (%) | 66.4 | 72.5 | 71.0 |
| FMA (°) | 24.0 | 20.0 | 21.5 |
| ODI (°) | 73.3 | 61.0 | 65.0 |
| Dental analysis | |||
| U1 to FH (°) | 116.5 | 127.0 | 116.5 |
| IMPA (°) | 90.0 | 79.0 | 83.0 |
| Interincisal angle (°) | 124.0 | 134.5 | 139.5 |
| FH to occlusal plane (°) | 10.5 | 0.5 | 3.5 |
| Soft tissue analysis | |||
| TVL to UL (mm) | 5.0 | 6.5 | 5.0 |
| TVL to LL (mm) | 2.5 | 6.5 | 3.0 |
| TVL to Pog′ (mm) | −3.0 | 6.0 | 4.5 |
| Nasolabial angle (°) | 85.0 | 106.5 | 110.0 |
The following treatment objectives were established: (1) correct the jaw discrepancies of the maxilla and the mandible, (2) correct the anterior crossbite and the posterior open bites, (3) improve the narrow maxillary intermolar widths and the torque of the mandibular posterior teeth, (4) improve overbite and overjet, (5) establish a stable Class I dental relationship, and (6) and improve facial and dental esthetics.
The first treatment option was to perform 2-jaw surgery to correct the patient’s skeletal discrepancies. The second option was to distalize the mandibular arch with ramal plates as TSADs after extraction of the mandibular left third molar. The patient selected the second treatment option with the ramal plates to avoid surgical treatment.
The patient was bonded with 0.022-in straight-wire fixed orthodontic appliances on the maxillary and mandibular dentitions with an initial wire of 0.016 copper-nickel-titanium. The wires were gradually changed to 0.019 × 0.025 stainless steel.
Distalization was continued for 6 months. Superimposition of the cone-beam computed tomography (CBCT) images taken before and after distalization shows the amount of molar distalization. A panoramic image was also reconstructed from the CBCT images after distalization ( Fig 6 ). The appliances were removed 27 months after the initial bracket placement. The prolonged treatment time was mainly because the patient missed several appointments. Maxillary and mandibular fixed retainers were bonded, and myofunctional therapy was recommended to control his tongue-thrust habit.
A Class I dental relationship was established. Normal overbite and overjet were obtained. Adequate interdigitation was achieved except on his second premolars because of the severity of his tongue-thrust habit ( Fig 7 ). The maxillary intermolar width increased from 38.5 to 41.0 mm.
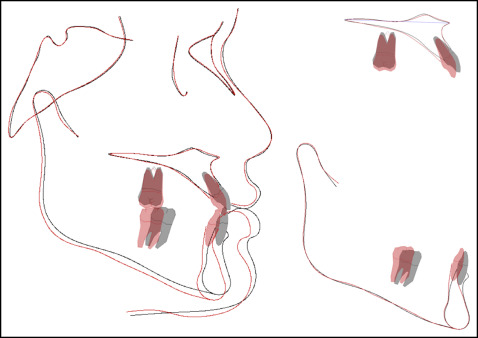
The posttreatment lateral cephalometric analysis and the superimposition showed that ANB increased from −4.0° to −2.5°, but his Class III profile was not improved significantly because of his prominent chin. The maxillary incisor inclinations were improved (U1-FH, from 127.0° to 116.5°). The mandibular incisor tip and pogonion were distalized by 2.5 and 1.5 mm, respectively. Lower anterior vertical height increased by 2 mm ( Figs 8 and 9 ; Table I ). The maxillary molars were extruded about 1.7 mm by up-and-down elastics. The mandibular first molar crown was distalized by 4.2 mm and the apex by 3.2 mm.
At the 33-month follow-up, the treatment effects were maintained, and the radiographs showed fairly stable results (ANB, −2.0°; U1-FH, 115.5°; IMPA, 82.5°; FMA, 21.5°). However, the patient still had a tongue-thrust habit, which opened his bite on the left second premolar and first molar. Myofunctional therapy to control his tongue thrust was stressed again. He was referred to his oral surgeon for an evaluation of his maxillary third molars ( Figs 10 and 11 ).
Patient 2
A 22-year-old man came with a chief complaint of “my lower teeth are sticking out.” He had had previous treatment with 4 first premolar extractions during adolescence ( Figs 12 and 13 ). He was slightly dolichofacial, with a symmetrical face and a straight profile. Intraorally, his maxillary central incisors showed edge-to-edge bites. He also had an anterior crossbite on his maxillary right lateral incisor and an open bite on his left lateral incisor. In addition, he had a tongue-thrust habit when swallowing. He had Class III canine and molar relationships on both sides with mild crowding on the maxillary arch and moderate crowding on the mandibular arch. Generalized gingival recession was seen on several teeth ( Fig 12 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


