Introduction
Several noninvasive methods are used for 3-dimensional (3D) morphologic facial and dental analysis to aid practitioners during diagnosis and treatment planning. Integrating dental and facial noninvasive 3D reproduction could improve the efficacy of treatment management.
Methods
Dental virtual model and soft-tissue facial morphology were digitally integrated from 11 adults with a 3D stereophotogrammetric imaging system (Vectra, Canfield Scientific, Fairfield, NJ). The digital 3D coordinates of 3 facial landmarks (N, nasion; Ftr, frontotemporale right; Ftl, frontotemporale left) and 3 dental landmarks (I, interincisor; Pr, PI, tips of the mesiovestibular cusps of the right and left first permanent premolars) were then obtained by using Vectra’s software. Additionally, the coordinates of the same 6 landmarks were digitized directly on each subject by using a 3D computerized electromagnetic digitizer (in vivo). Seven linear measurements were made between the occlusal plane (Pr-I-Pl) and the facial landmarks (Ftr-N-Ftl). The accuracy and reliability of the reconstruction were tested by in-vivo measurements and repeated acquisitions.
Results
The greatest mean relative error of measurements was smaller than 1.2%. No significant differences in repeatable reproductions were found.
Conclusions
Integration of facial stereophotogrammetry acquisition and dental laser scan reproduction is possible with marginal error.
Clinical assessments based on anthropometric studies offer a significant change in the process of diagnosis for various syndromes, giving support to plastic and orthognathic surgery, detecting normal and abnormal growth, and providing information for planning and evaluating medical procedures and treatments. Studies with three-dimensional (3D) reconstructions reported accurate and reliable techniques for facial analyses, aiding clinicians in planning more effective treatments.
Several noninvasive methods such as laser scanning, magnetic resonance imaging, contact digitizers, Moiré stripes, and stereophotogrammetry are used for 3D morphologic facial analysis. Stereophotogrammetry is a system that uses 2 or more cameras to record several simultaneous photos from different viewpoints to obtain a digital 3D image. This technique is a promising method of soft-tissue evaluation that allows reliable analysis of craniofacial deformities, providing fundamental parameters to plan and evaluate treatments and maxillofacial surgery. Current technology also allows digitizalation of dental models in 3D space, and the association between the digital dental cast and the 3D facial images could allow the clinician to analyze the relationship between soft tissues and dental arches, avoiding when possible the use of x-rays.
Rangel et al recently proposed the integration of a digital dental cast into a 3D facial picture. According to the average distance between the matched areas (anterior teeth) in a patient, the method was reported to be reliable, but larger studies are necessary to verify whether matching between the digital dental cast and the 3D facial image could correspond to the correct position of the whole dental arches.
Because the matching between the 3D face and the digital casts with stereophotogrammetric systems must use the anterior teeth as the reference, any displacement or inclination of the digital dental arch would add a position error in the posterior region. Thus, some questions arise. Is the occlusal plane in the correct position? Are the posterior teeth in the correct position? Therefore, the aims of this study were to elaborate and validate the matching between digital dental casts and stereophotogrammetric images as a noninvasive 3D reconstruction of dentofacial structures in healthy subjects, analyzing distances between the occlusal plane and the facial landmarks.
Material and methods
Healthy subjects were selected to have their maxillary dental casts digitized by laser scanning and their 3D facial soft-tissue acquisitions merged into 1 file. Seven linear distances through facial and dental landmarks were measured and compared between the in-vivo and the virtual reproductions to quantify the accuracy of the final 3D reconstruction.
A group of 11 healthy volunteers, 4 men and 7 women, from 20 to 31 years of age, with no history of craniofacial trauma, no congenital anomalies, and full maxillary and mandibular dental arches, were selected. All procedures were noninvasive and were carried out with minimal disturbance to the subjects, who were previously informed about the procedures and gave written consent to the investigation, according to the principles outlined in the Declaration of Helsinki.
For each subject, a maxillary dental reproduction was obtained by an irreversible hydrocolloid (Tropicalgin, Zhermack SpA, Badia Polesine, Italy) and cast with a type 3 model dental stone (Elite model, Zhermack SpA). Using a commercial laser scanner (D100, Imetric 3D, Courgenay, Switzerland), the dental casts were digitized, and the appropriate files were imported into the stereophotogrammetric software.
The soft tissues’ facial morphology was acquired with a 3D stereophotogrammetry imaging system (Vectra 3D, Canfield Scientific, Fairfield, NJ). This is a modular 3D system designed to capture and process stereo images. It consists of 2 pods, including 3 cameras (2 black and white, and 1 color) and a projector in each pod.
The system records synchronized pairs of 2-dimensional images of the subjects. With dedicated software, the information is used to work out the 3D reconstructions that subsequently can be processed, analyzed, manipulated, and measured. The reproducibility of stereophotogrammetric technology has been well documented.
Before each acquisition, 3 soft-tissue landmarks (N, nasion; Ftr, frontotemporale right; Ftl, frontotemporale left) were marked on the face with black liquid eye liner for further analysis. For each subject, 2 sets of 3D facial images were obtained: with open lips (with cheek retractors) with visible frontal teeth and with the teeth in occlusion and closed lips.
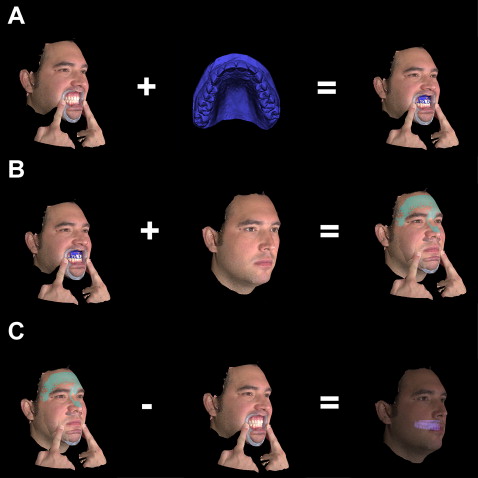
To obtain virtual dentofacial reproductions, the 3D facial images and the corresponding maxillary digital dental arch were matched by using Vectra’s software tools. The matching process needed 3 steps ( Fig 1 ).
- 1.
The digital dental cast was merged with the open-lips facial acquisition, and anterior dental landmarks, present in both acquisitions, were used as fiducial points.
- 2.
The image with closed lips was introduced to be related to the open-lips image; the facial soft-tissue landmarks N, Ftr, and Ftl were used as fiducial points.
- 3.
The open-lips acquisition was removed from the file, obtaining a final digital image ( Fig 2 ), with the dental cast and the facial reconstruction with closed lips in the relevant 3D positions.

Fig 2 Three-dimensional teeth-facial reproduction
The matching of the 2 surfaces was obtained with 2 techniques: an initial approximate alignment was performed, overlapping the 3 fiducial points recognizable in both surfaces. The procedure was then improved by using the “register surface” control in the Vectra software.
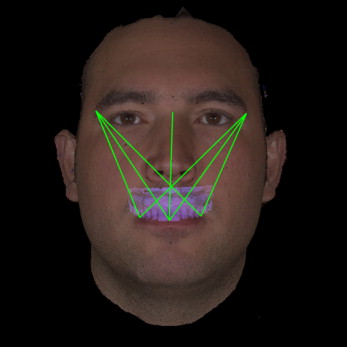
To verify the accuracy of the virtual full reproduction, the 3D coordinates of the 3 facial (N, Ftr, and Ftl) and the 3 dental (I, interincisor; Pr and Pl, tips of the vestibular cusps of right and left first permanent first premolars) landmarks were obtained directly on each subject by using a 3D computerized electromagnetic digitizer (3Draw, Polhemus, Colchester, Vt) with a resolution of 0.0005 cm per centimeter of range.
Seven linear measurements were then mathematically computed from the 3D coordinates and calculated with Euclidean geometry ( Table I ). The same linear distances were also obtained from the 3D digital reproduction by using Vectra’s software tools ( Fig 3 ).
| In vivo (mm) | Virtual (mm) | MAD | CI | TEM (mm) | REM (%) | Wilcoxon test P value | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Distance | Mean | SD | Mean | SD | (mm) | (mm) | (mm) | |||
| Ftr-Pr | 86.9 | 6.5 | 87 | 6.1 | 0.8 | 0.44 | 1.16 | 0.7 | 0.9 | 0.66 |
| Ftr-Pl | 106.7 | 4.1 | 106.9 | 3.4 | 1.1 | 0.55 | 1.65 | 1 | 1 | 0.53 |
| N-I | 85.8 | 19.9 | 86.3 | 20.1 | 0.7 | 0.45 | 0.95 | 0.6 | 0.9 | 0.051 |
| Ftl- Pl | 87.4 | 5.4 | 87.8 | 5.5 | 0.9 | 0.65 | 1.15 | 0.7 | 1.1 | 0.29 |
| Ftl-Pr | 106 | 3.6 | 107 | 3.7 | 1.2 | 0.7 | 1.7 | 1 | 1.1 | 0.03 ∗ |
| Ftr-I | 101.9 | 5.8 | 102.1 | 5.1 | 0.9 | 0.5 | 1.3 | 0.8 | 0.9 | 0.59 |
| Ftl-I | 100.8 | 5.9 | 101.8 | 5.9 | 1.2 | 0.79 | 1.61 | 1 | 1.2 | 0.03 ∗ |
To investigate the reliability of matching between the images, the merging procedures described above were done twice, and the distances reported in Table I were calculated on each matching.
Because the merged images were made with 2 photos (closed and open lips, Fig 1 , B ), to assess the accuracy of Vectra’s matching, a random area comprising forehead, temples, and nose was selected for each closed-lips photograph, and the distance from the respective open-lips pictures was evaluated. Ideally, this part of the face should not move with open lips.
Statistical analysis
Wilcoxon signed rank tests were made between the distances computed in vivo and on the virtual reproduction to detect possible systematic errors. P values less than 0.05 were considered significant.
Mean absolute difference (MAD), technical error of measurement (TEM), and relative error magnitude (REM) were calculated to quantify the precision of our protocol. MAD is the average of absolute differences between the values of 2 sets of measurements; TEM or Dahlberg’s error was used to evaluate the random error. The REM was obtained by dividing the MAD for a variable by the grand mean for that variable and multiplying the result by 100; it represents an estimate of error magnitude relative to the size of the measurement.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


