CHAPTER 2 Differential tooth movement
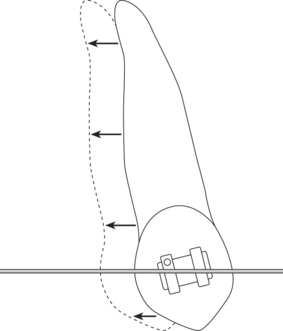
It is customary, in contemporary fixed appliance orthodontics, to work towards finishing angulations from the outset of treatment. This is because edgewise derived brackets, in common use today, dictate this upon the orthodontist by exerting mesio-distal second order root forces from the time of first engagement with an archwire. The very design of such a bracket therefore imposes a treatment regimen of bodily movement (Fig. 2.1) and with it, over many years, has grown the widespread assumption that this is the way teeth require to be moved.
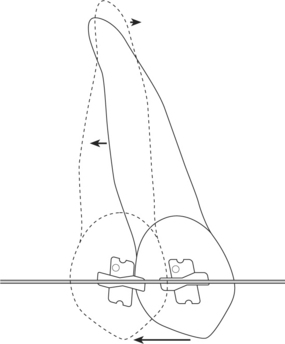
By complete contrast, a bracket designed for differential tooth movement will not impart root-angulating forces when an archwire is engaged. Instead, the crown will be able to tip in the direction of desired tooth movement, essentially leaving the root apex to trail behind (Fig. 2.2). Obviously, such simple free tipping requires far less force and anchorage than moving the same tooth bodily, although this would in itself amount to incomplete treatment. However, it makes initial decrowding and reduction of big overjets dramatically easy, as well as rapid, together with the attainment of a Class I buccal segment occlusion. Both are achieved early in treatment. This in turn lends stability to the subsequent root uprighting process, both by establishing a strong interdigitation and by bringing the labial segments within the safety of normal lip control, as opposed to the adverse influences of persistent lip trapping.
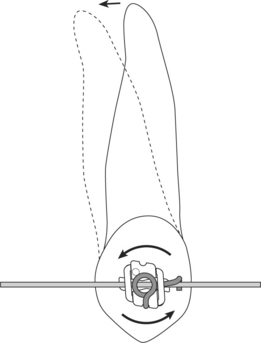
Of course, this constitutes only half the treatment and the root uprighting, which necessarily follows, may occupy the latter half of the total treatment time (Fig. 2.3). Inevitably, this has anchorage consequences, which will be discussed in Chapter 14. However, it is a striking feature of differential tooth movement that total anchorage requirements, and duration of treatment, seem significantly less than with straight-wire or edgewise systems, particularly in difficult cases.1,2 No doubt protagonists for the conventional will wish to challenge this claim, on grounds of lack of scientific evidence; indeed it would be difficult to measure anchorage objectively. Nevertheless, on clinical evidence, it is unarguable.
Why this should be so remains unexplained. Following treatment of any m/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


