Introduction
Miniscrews are frequently used for skeletal anchorage during edgewise treatment, and their clinical use has been verified. However, their disadvantage is an approximately 15% failure rate, which is primarily attributed to the low mechanical stability between the miniscrew and cortical bone and to the miniscrew’s close proximity to the dental root. To solve these problems, we developed a novel spike-like auxiliary skeletal anchorage device for use with a miniscrew to increase its stability.
Methods
The retention force was compared between miniscrews with and without the auxiliary skeletal anchorage device at each displacement of the miniscrew. The combined unit was also implanted into the bones of 2 rabbits in vivo, and implantation was visually assessed at 4 weeks postoperatively while the compression force was applied.
Results
The retention force of the combined unit was significantly and approximately 3 to 5 times stronger on average than that of the miniscrew alone at each displacement. The spiked portion of the auxiliary anchorage device embedded into the cortical bone of the hind limb at approximately a 0.3-mm depth at 4 weeks postimplantation in both rabbits.
Conclusions
The auxiliary skeletal anchorage device may increase miniscrew stability, allow a shortened miniscrew, and enable 3-dimensional absolute anchorage. Further evaluation of its clinical application is necessary.
Highlights
- •
We developed a novel spike-like auxiliary skeletal anchorage device.
- •
This device enables automatic embedding of the spiked portion into the cortical bone.
- •
This device enhances miniscrew stability 3 to 5 times that of a miniscrew alone.
- •
This device allows a shortened miniscrew.
- •
This device enables 3-dimensional absolute anchorage.
Both miniscrews and miniplates have been used in clinical orthodontic practice to provide skeletal anchorage. Miniplates do offer a lower failure rate in comparison with other skeletal anchorage devices such as miniscrews ; however, the devices are disadvantaged by the significantly increased patient discomfort, a highly complex implantation procedure, and greater invasiveness because of the required flap surgery.
The miniscrew has recently come into use for skeletal anchorage during edgewise treatment and is the most frequently implanted of all skeletal anchorage devices. Miniscrews have enabled numerous orthodontic treatments that were difficult with conventional appliances: eg, mesial movement of a molar in a patient with oligodontia, distal movement of the maxillary and mandibular teeth, and improvement of an open bite caused by intruding posterior teeth. In addition, miniscrews have often been used to provide 2-dimensional absolute anchorage during edgewise treatment.
Currently, the usefulness of miniscrews has been conclusively shown with a high level of evidence, but the devices have some disadvantages. Miniscrews require extremely precise implantation when placed into the narrow space between 2 dental roots. Cone-beam computed tomography is not recommended to examine the space between the roots and the cortical bone thickness because of the high radiation exposure, particularly in growing patients. Most critically, miniscrews have an approximately 15% failure rate on average ; with this high rate of failure, in a patient population implanted with 4 miniscrews each, approximately 50% of the patients will experience failure in more than 1 miniscrew, ultimately leading to reimplantation.
Two primary factors are implicated in miniscrew failure. One is the low mechanical stability between the miniscrew and the cortical bone. This results in even higher failure rates in patients with a high mandibular plane angle and in growing patients than in patients with a low or an average mandibular plane angle and adult patients. Another factor is the close proximity of the miniscrew to the dental root. Prevention of miniscrew failure thus requires meeting 2 crucial conditions: increased mechanical stability, achieved by increasing the contact area between the miniscrew and the cortical bone, and prevention of root proximity by shortening the miniscrew. However, increasing the miniscrew diameter to enhance the mechanical stability also increases the risk of root proximity, whereas decreasing the miniscrew diameter decreases the risk of root proximity. As a result, no currently available miniscrews or skeletal anchorage devices meet these conditions while remaining minimally invasive. Accordingly, we developed an auxiliary skeletal anchorage device that is used in conjunction with a miniscrew to increase its stability, enabling 3-dimensional absolute anchorage and ultimately helping to avoid root proximity with a shorter miniscrew. Furthermore, we evaluated the mechanical stability force between artificial bone and the combined miniscrew and auxiliary skeletal anchorage device, and assessed the degree of embedding of the auxiliary device after the compression force was applied for 4 weeks through a silicone ring between the auxiliary device and the miniscrew head.
Material and methods
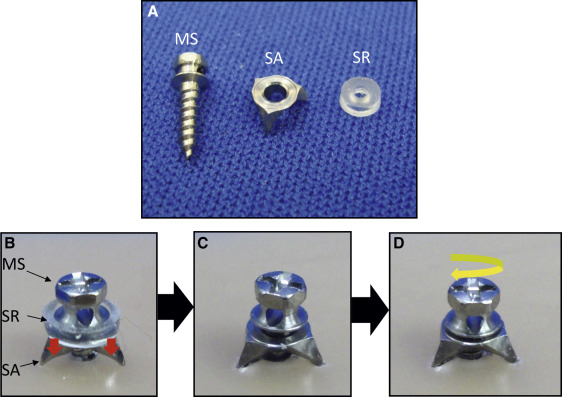
To increase the mechanical stability between the miniscrew and the cortical bone, we developed an auxiliary skeletal anchorage device made of titanium alloy (raw material, Ti6Al4V; ASTM F136-96) comprising 2 portions: a washer portion that receives the force from the screw head and transfers it through the silicone at the first stage of implantation, and a spiked portion that contacts and slightly embeds into the cortical bone during the first stage: ie, as the compression force was applied through the silicone ring between the auxiliary device and the miniscrew head ( Fig 1 , A-C ). During the first stage of implantation, a silicone ring (thickness, 1.0 mm; Durometer Shore A, 18; tensile strength, 4.14 MPa [600 psi]; tearing strength, 45; tensile elongation, 700%; elastic modulus, 0.82 MPa; Bitec Global Group, Tokyo, Japan) was placed between the screw head and the washer portion of the auxiliary skeletal anchorage device. A preliminary study (data not shown) showed that an approximately 1 to 2 N force is delivered to the spiked portions of the auxiliary skeletal anchorage device through the silicone ring, allowing embedding into the cortical bone over time as the compression force is applied through the silicone ring between the auxiliary device and the screw head. One month after embedding the spiked portion of the miniscrew into the bone to approximately a 0.3-mm depth, the silicone ring was removed, and the miniscrew was further tightened to allow the spiked portion to compress more securely to the cortical bone ( Fig 1 , D ).
The artificial bone blocks (Sawbones; Pacific Research Laboratories, Vashon Island, Wash) included cancellous bone constructed from 0.08 g per millileter (5 pcf) density cellular rigid polyurethane foam and 1-mm-thick cortical bone constructed from 0.64 g per milliliter (40 pcf) laminated rigid polyurethane foam. The constructed blocks measured 2.54 cm (1 in) in length and width, and 4.57 cm (1.8 in) in height ( Fig 2 , A ).
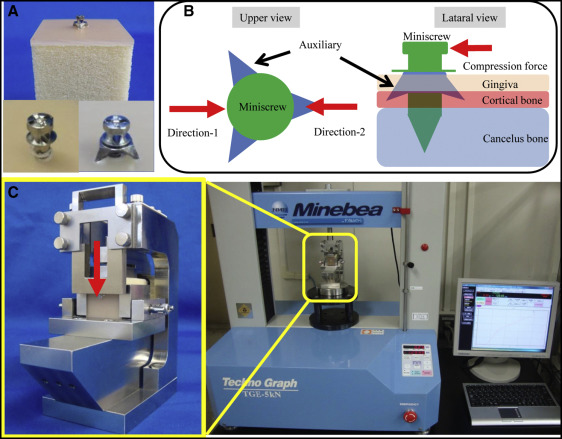
For the lateral displacement test, the mechanical retention force between the skeletal anchorage and the artificial bone was determined using titanium alloy miniscrews measuring 1.6 mm in diameter and 6.0 mm in length (Dual-Top; Jeil Medical, Seoul, Korea). Two groups comprising 10 miniscrews each were implanted en masse into artificial bone blocks using a driver machine (Orthonia 111-ED-010; Jeil Medical); 1 group was implanted with an auxiliary skeletal anchorage device (auxiliary group) and 1 without the auxiliary device (nonauxiliary group). The spiked portion of the auxiliary skeletal anchorage device was implanted into the cortical region of the artificial bone to a depth of 0.3 mm. The depths of miniscrew implantation in both groups were then adjusted until they were equal between the groups. To determine the mechanical retention force, the displacement of the miniscrew head was measured after application of a compression force delivered from 2 directions ( Fig 2 , B ) using a compression test machine (TGE-5kN; Minebea, Nagano, Japan) set at a load of 5.0 kN and a compression velocity of 0.5 mm per minute ( Fig 2 , C ). The compression force was delivered in 2 directions parallel to the artificial bone surface until each miniscrew moved 0.01, 0.02, and 0.03 mm from its initial position. The resulting force was calculated with software (SR-06-001 version 3.400; Minebea).
A miniscrew with an auxiliary skeletal anchorage device was implanted into 2 New Zealand white rabbits, 1 male and 1 female, aged 14 weeks and weighing approximately 3 kg. All surgical procedures were performed under general (1 mg/kg ketamine and 2 mg/kg xylazine) and local (2% lidocaine with 1:80,000 epinephrine) anesthesia. Before surgery, each rabbit was placed under general anesthesia and showed no response to pain stimulation. One hind limb was shaved and aseptically cleansed with povidone-iodine and 70% ethanol. A flap was reflected on each femur using a periosteal elevator, and the miniscrews were implanted at least 10 mm apart with a driver machine.
At 4 weeks postimplantation, each animal was killed by a lethal dose of pentobarbital, and the implanted limb was isolated. The specimen was visually examined to determine whether automatic embedding of the auxiliary skeletal anchorage device occurred during the intervening 4 weeks after implantation. This animal experimental protocol was approved by the institutional experimentation committee of Kagoshima University (number D13010).
Statistical analysis
The retention force in each displacement was compared between the 2 study groups using the Mann-Whitney U test. Data were analyzed with statistical software (version 10.0; IBM, Armonk, NY), and statistical significance was designated at α <0.05.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


