Introduction
The aim of this study was to compare the dentoskeletal changes of patients with Class II Division 1 malocclusion treated with either the Jasper jumper appliance or the activator-headgear combination, both associated with fixed appliances.
Methods
The sample comprised 72 subjects with Class II Division 1 malocclusion divided into 3 groups: group 1 included 25 subjects treated with fixed appliances and the force modules of the Jasper jumper at an initial mean age of 12.72 years, group 2 included 25 subjects treated with the activator-headgear combination followed by fixed appliances at an initial mean age of 11.07 years, and group 3 included 22 untreated subjects at an initial mean age of 12.67 years. Initial cephalometric characteristics and dentoskeletal changes were compared with analysis of variance.
Results
Both experimental groups had similar dentoskeletal changes: restrictive effect on the maxilla, clockwise mandibular rotation and a slight increase in anterior face height, retrusion of the maxillary incisors, distalization of the maxillary molars, protrusion of the mandibular incisors, extrusion of the mandibular molars, and significant improvements of the maxillomandibular relationship, overjet, overbite, and the molar relationship.
Conclusions
The effects of the Jasper jumper and the activator-headgear combination followed by fixed orthodontic appliances were similar in Class II malocclusion treatment.
A common strategy in the treatment of Class II Division 1 malocclusions in growing patients is a 2-step approach. In the first phase of treatment, the sagittal jaw relationship is normalized. The Class II malocclusion is transformed to a Class I malocclusion. In the second phase of treatment, tooth positions are adjusted, usually with fixed appliances. Correction of the sagittal jaw relationship can be achieved in several ways. Removable functional appliances, such as the activator, change a Class II relationship by the transmission of soft-tissue tension to the dentition. This is achieved by positioning the mandible anteriorly with the appliance. In Jasper jumper therapy, fixed appliances with flexible intraoral force modules are used in the first phase of treatment.
Only 2 studies in the English literature have compared the initial dentoskeletal effects between the Jasper jumper and the activator-headgear combination in Class II malocclusion treatment. However, 1 study had no control group. Sari et al concluded that the activator-headgear appliance was more effective on the mandible, whereas the jumper appliance was mainly active on the maxilla. Weiland et al studied 72 Class II patients treated with either the Herren activator associated with headgear or the Jasper jumper appliance. Corrections of overjet and molar relationship were more evident in patients treated with the Jasper jumper compared with the activator.
De Oliveira et al evaluated the dentoskeletal effects of the Jasper jumper associated with cervical headgear followed by edgewise therapy in the treatment of Class II malocclusion. They concluded that the headgear corrected the Class II malocclusion mostly by restriction of maxillary anterior displacement and maxillary dentoalveolar effects. Correction of the Class II malocclusion with the Jasper jumper was largely due to mandibular dentoalveolar effects rather than skeletal effects.
No previous clinical investigation has evaluated the overall effects of the Jasper jumper and compared it with activator-headgear combination; both were associated with edgewise therapy in the treatment of Class II malocclusion. Therefore, the purpose of this clinical study was to investigate the dentoskeletal changes in 2 groups of patients with Class II Division 1 malocclusion treated with either the Jasper jumper appliance or the activator-headgear combination, both associated with fixed appliances. These groups were compared with a control group of untreated subjects with similar malocclusions.
Material and methods
This study was approved by the ethics in research committee of the Bauru Dental School, University of São Paulo, Brazil, and all subjects signed informed consent. This was a comparison of the effects of 2 approaches for Class II Division 1 malocclusion correction. The study sample comprised 72 subjects (50 treated, 22 untreated). Fifty consecutively treated patients in the orthodontic department at Bauru Dental School were evaluated in this clinical study. Subject selection was based exclusively on the initial anteroposterior molar relationship, regardless of any other dentoalveolar or skeletal cephalometric characteristics. All patients met the following inclusion criteria: (1) Class II Division 1 malocclusion with bilateral Class II molar relationship (minimum severity of one half Class II molar relationship ), (2) no craniofacial syndromes or systemic diseases, (3) no tooth agenesis or missing permanent teeth, and (4) mandibular arch with minimal or no crowding.
The Jasper jumper group (group 1) included 25 subjects (13 boys, 12 girls) treated with fixed appliances and the force modules of the Jasper jumper appliance. All patients were in the early permanent dentition with all first permanent molars, and first and second premolars erupted. Their initial mean age was 12.72 years (SD, 1.21; range, 10.32-14.84 years), and their final mean age was 14.88 years (SD, 1.20; range, 12.74-16.90 years), treated for a mean period of 2.15 years (SD, 0.30). These subjects had an initial mean ANB angle of 5.38° (SD, 2.87°) and an initial mean overjet of 6.24 mm (SD, 2.21 mm). This group was collected and treated by 1 operator (K.J.R.S.L.).
The activator-headgear combination followed by fixed appliances group (group 2) consisted of 25 subjects (8 boys, 17 girls). All patients were in the early permanent dentition with all first permanent molars, and first and second premolars erupted. This group had an initial mean age of 11.07 years (SD, 1.17; range, 8.57-13.61 years) and a final mean age of 14.19 years (SD, 1.30; range, 12.15-16.79 years) and was followed for a mean period of 3.21 years (SD, 1.29). These subjects had an initial mean ANB angle of 6.42° (SD, 1.29°) and an initial mean overjet of 8.69 mm (SD, 2.50 mm).
The control group (group 3) was obtained from the Longitudinal Growth Study files at Bauru Dental School. This group comprised 22 subjects (12 boys, 10 girls) with Angle Class II Division 1 malocclusion and no orthodontic treatment, at an initial mean age of 12.67 years (range, 11.21-13.98 years) and a final mean age of 14.80 years (SD 1.71), who were longitudinally followed for a mean period of 2.13 years (SD, 1.64). These subjects had an initial mean ANB angle of 4.11° (SD, 1.83°) and an initial mean overjet of 4.70 mm (SD, 1.60 mm).
In the Jasper jumper group, standard edgewise brackets with a 0.022 × 0.025-in slot were used, and bands were placed with a transpalatal arch in the maxillary arch to increase stability. For leveling and aligning, the sequence of wires used was 0.016-in nickel-titanium archwire, and 0.018-, 0.020-, and 0.018 × 0.025-in stainless steel archwires. During this phase, the Jasper jumper was installed ( Fig 1 ). The mandibular arch was tied back to the first or second molars. In the maxillary arch, the jumper was attached to the headgear tube of the first molars as prescribed by the manufacturer with a ball-pin attachment. In the mandibular arch, the jumper was attached to the rectangular 0.018 × 0.025-in stainless steel archwire with a ball-pin attachment over the mandibular canine bracket from the distal side. Jasper jumpers were selected according to the manufacturer’s instructions. The patients were seen every 4 weeks, and the appliances were activated every 8 weeks. The appliance was removed when a Class I or overcorrected Class I canine and molar relationship was achieved. The mean treatment time with the Jasper jumper was 7 months (range, 3-12 months). After removal of the jumpers, the corrected anteroposterior relationship was retained with 5/16-in Class II elastics for a mean period of 4 months (range, 1-8 months), with a daily recommended use of 14 hours. After removal of the fixed orthodontic appliances, a Hawley plate was used in the maxillary arch, and a canine-to-canine bonded retainer was used in the mandibular arch. A bionator was also used at night for 12 months.

The activator-headgear appliance consisted of a bimaxillary block of acrylic with a screw expander on top, a maxillary labial bow (0.7 mm), and Adams clasps on the maxillary first molars. The incisal third of the mandibular incisors was capped with acrylic to prevent extreme labial tipping. Headgear bows were incorporated into the interocclusal acrylic in the premolar area ( Figs 2 and 3 ). The construction bite was taken with the mandible protruded in an edge-to-edge incisor relationship, and the interocclusal space was increased to 7 mm. In patients with large overjets, a 2-step activation was performed. The outer bow was tilted 15° upward from the occlusal plane, exerting 400 g of force in each side with an average wear of 15 hours per day. The patients underwent an orthopedic treatment with the activator-headgear combination for a mean period of 13.6 months (SD, 3.9; range, 3.8-18.6 months). They were instructed to use the appliances for 15 hours a day. Cooperation was evaluated by the monthly changes expected. After obtaining a normal anteroposterior relationship with this appliance, fixed standard edgewise appliances were installed ( Fig 4 ). Leveling and aligning followed the usual sequence: 0.016-in nickel-titanium archwire, and 0.018-, 0.020-, and 0.018 × 0.025-in stainless steel archwires. Most patients (60%) used the Kloehn headgear for 14 hours a day during fixed appliance treatment. Others (40%) used Class II elastics for active retention for 14 hours a day. These devices were used during 70% of the fixed appliance phase that lasted 24.9 months. After removal of the fixed orthodontic appliances, a Hawley plate was used in the maxillary arch, and a canine-to-canine bonded retainer was used in the mandibular arch. All patients were treated without extractions.


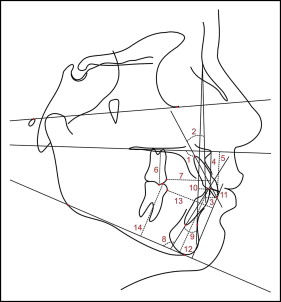
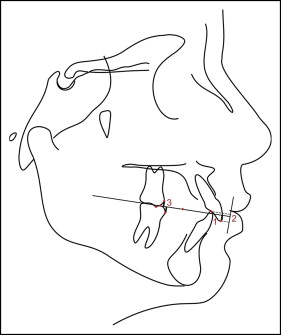
Lateral cephalograms of each patient were taken before and after treatment. Anatomic tracings of the lateral cephalograms and landmark locations were manually conducted and digitized (AccuGrid XNT, model A30TL.F; Numonics, Montgomeryville, Pa) by 1 investigator (K.J.R.S.L.). These data were then stored in a computer and analyzed with software (version 7.02; Dentofacial Software, Toronto, Ontario, Canada). This software corrected the magnification factors (6%, 7.9%, and 9.8%) of the radiographic images. The less usual cephalometric variables are defined in Table I and illustrated in Figures 5 and 6 .
| 1.PP (°): angle formed by the maxillary incisor’s long axis and the palatal plane (PP) |
| 1-PP (mm): linear distance from the maxillary central incisor edge projected perpendicularly to the PP |
| 6-PP (mm): linear distance from the mesiovestibular cusp of the maxillary first molar projected perpendicularly to the PP |
| 6-ANS perp (mm): linear distance from the maxillary first molar mesial point to the ANS perp line (line perpendicular to the PP passing through the anterior nasal spine) |
| 1.NA (°): angle formed by the maxillary incisor’s long axis and the NA line |
| 1-NA (mm): linear distance between the most anterior point of the maxillary central incisor and the NA line |
| IMPA (°): angle formed by the mandibular incisor’s long axis and the mandibular plane (GoMe) |
| 1-GoMe (mm): linear distance between the mandibular incisor edge perpendicular to GoMe |
| A-N perp (mm): linear distance from Point A to the Nperp line (line perpendicular to the Frankfort plane passing through N) |
| Pog-Nperp (mm): linear distance from Pog to the Nperp line |
| 1.NB (°): angle formed by the mandibular incisor’s long axis and the NB line |
| 1-NB (mm): linear distance between the most anterior point of the mandibular central incisor and the NB line |
| 6-Pog-perp (mm): linear distance between the mandibular first molar’s mesial point to the Pog-perp line (line perpendicular to the mandibular plane Go-Me passing through Pog) |
| 6-GoMe (mm): linear distance between the mesiovestibular cusp of the mandibular first molar perpendicular to GoMe |
Thirty lateral cephalograms were randomly selected, retraced, redigitized, and remeasured by the same examiner (K.J.R.S.L.) after a 30-day interval. Casual and systematic errors were calculated by comparing the first and second measurements with Dahlberg’s formula and dependent t tests, respectively, at a significance level of 5%.
Statistical analysis
Chi-square tests were used to check the compatibility among the 3 groups regarding sex distribution and severity of the initial Class II molar relationship.
Analysis of variance (ANOVA) and Tukey tests were used for intergroup comparisons of the initial and final ages and cephalometric statuses, and treatment or observation changes.
Because the activator-headgear group had a significantly lower initial age and a longer treatment time, the treatment changes were annualized according to the Jasper jumper treatment time. Therefore, all patients in this group had their individual treatment changes for each variable divided by their treatment time, and then multiplied by the mean treatment time of group 1.
All statistical analyses were performed with Statistica software (statistical software for Windows, version 6.0; Statsoft, Tulsa, Okla). The results were considered statistically significant at P <0.05.
Results
There were no statistically significant systematic errors, and the casual errors varied from 0.23 mm (1-PP) to 1.36° (IMPA).
The groups were compatible regarding sex distribution ( Table II ).
| Sex | Group 1, Jasper jumper (n = 25) | Group 2, activator-headgear (n = 25) | Group 3, control (n = 22) | P |
|---|---|---|---|---|
| Female | 12 (48%) | 17 (68%) | 10 (45%) | 0.2251 χ 2 = 2.9825 |
| Male | 13 (52%) | 8 (32%) | 12 (55%) |
Initial Class II anteroposterior severity was significantly less in the control group, but similar between the experimental groups ( Tables III and IV ).
| Severity of Class II | Group 1, Jasper jumper (n = 25) | Group 2, activator-headgear (n = 25) | Group 3, control (n = 22) | P |
|---|---|---|---|---|
| ¼ Class II | 0 | 0 | 4 (18%) | 0.0006 χ 2 = 23.6801 |
| ½ Class II | 4 (16%) | 4 (16%) | 11 (50%) | |
| ¾ Class II | 9 (36%) | 6 (24%) | 4 (18%) | |
| Complete Class II | 12 (48%) | 15 (60%) | 3 (14%) |
| Severity of Class II | Group 1, Jasper jumper (n = 25) | Group 2, activator-headgear (n = 25) | P |
|---|---|---|---|
| ¼ Class II | 0 | 0 | 0.6271 χ 2 = 0.9333 |
| ½ Class II | 4 (16%) | 4 (16%) | |
| ¾ Class II | 9 (36%) | 6 (24%) | |
| Complete Class II | 12 (48%) | 15 (60%) |
The activator-headgear group had a significantly lower initial age and a longer treatment time than did the other groups ( Table V ).
| Variable (y) | Group 1, Jasper jumper (n = 25) | Group 2, activator-headgear (n = 25) | Group 3, control (n = 22) | P | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Initial age | 12.72A | 1.21 | 11.07B | 1.17 | 12.67A | 0.75 | 0.0000 |
| Final age | 14.88 | 1.20 | 14.19 | 1.30 | 14.80 | 1.71 | 0.1753 |
| Observation interval | 2.15A | 0.30 | 3.21B | 1.29 | 2.13A | 1.64 | 0.0025 |
The activator-headgear group had significantly greater mandibular retrusion, and smaller mandibular length and posterior facial height than did the other 2 groups ( Table VI ). The experimental groups had significantly greater Class II anteroposterior discrepancies and facial convexities than did the control group. The maxillary incisors had significantly greater protrusion in the headgear-activator group, and the maxillary molars had a significantly greater mesial position in the experimental groups. Overjet was progressively and significantly smaller from the activator-headgear, followed by the Jasper jumper and control groups. Class II molar relationship was significantly greater in the experimental groups than in the control group.
| Variable | Group 1, Jasper jumper (n = 25) | Group 2, activator-headgear (n = 25) | Group 3, control (n = 22) | P | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Maxillary components | |||||||
| SNA (°) | 82.58 | 3.38 | 81.49 | 3.25 | 81.65 | 3.29 | 0.4595 |
| A-Nperp (mm) | 1.34 | 3.63 | 0.48 | 2.81 | 0.69 | 2.55 | 0.5823 |
| Co-A (mm) | 85.87 | 4.47 | 84.90 | 4.12 | 87.01 | 4.42 | 0.2544 |
| Mandibular components | |||||||
| SNB (°) | 77.21A | 2.56 | 75.06B | 2.85 | 77.54A | 3.67 | 0.0113 |
| P-Nperp (mm) | −4.74A,B | 5.01 | −7.92A | 5.61 | −4.12B | 4.15 | 0.0220 |
| Co-Gn (mm) | 106.30A | 5.13 | 102.57B | 5.21 | 106.80A | 5.81 | 0.0147 |
| Maxillomandibular relationship | |||||||
| ANB (°) | 5.38A,B | 2.87 | 6.42A | 1.29 | 4.11B | 1.83 | 0.0018 |
| Wits (mm) | 1.75A | 2.52 | 2.36A | 2.16 | −0.16B | 2.58 | 0.0020 |
| NAP (°) | 8.97A,B | 7.30 | 11.27A | 4.36 | 6.91B | 4.70 | 0.0354 |
| Growth pattern | |||||||
| SN.GoGn (°) | 31.12 | 4.01 | 32.89 | 3.63 | 30.83 | 4.58 | 0.1686 |
| FMA (°) | 24.72 | 3.85 | 26.12 | 4.56 | 24.17 | 2.83 | 0.2035 |
| LAFH (mm) | 61.81 | 4.22 | 60.33 | 3.66 | 60.70 | 3.95 | 0.3953 |
| S-Go (mm) | 69.34A,B | 4.93 | 66.18A | 4.32 | 69.65B | 4.88 | 0.0217 |
| Maxillary teeth | |||||||
| 1.NA (°) | 24.49 | 7.30 | 27.29 | 7.40 | 23.30 | 6.02 | 0.1350 |
| 1-NA (mm) | 4.64 | 2.57 | 5.08 | 2.41 | 3.46 | 1.76 | 0.0534 |
| 1.PP (°) | 114.48 | 6.91 | 116.71 | 8.01 | 113.11 | 6.06 | 0.2172 |
| 1-ANS perp (mm) | −1.85A | 2.64 | 0.16B | 3.23 | −3.56A | 2.56 | 0.0001 |
| 1-PP (mm) | 26.51 | 2.61 | 25.79 | 2.37 | 26.58 | 2.53 | 0.4779 |
| 6-ANS perp (mm) | −30.65A | 2.82 | −29.86A | 2.93 | −32.57B | 2.31 | 0.0036 |
| 6-PP (mm) | 20.95 | 2.12 | 19.60 | 1.88 | 20.57 | 2.06 | 0.0573 |
| Mandibular teeth | |||||||
| IMPA (°) | 97.88 | 7.52 | 96.51 | 4.51 | 94.95 | 4.71 | 0.2323 |
| 1.NB (°) | 28.65 | 5.83 | 26.74 | 5.20 | 25.66 | 5.08 | 0.1615 |
| 1-NB (mm) | 5.10 | 2.06 | 4.11 | 1.81 | 3.98 | 1.80 | 0.0872 |
| 1-GoMe (mm) | 38.63 | 2.84 | 37.21 | 2.44 | 37.20 | 2.40 | 0.0885 |
| 6-Pog-perp (mm) | −29.21 | 2.19 | −29.40 | 2.65 | −30.15 | 2.09 | 0.3583 |
| 6-GoMe (mm) | 27.91 | 2.31 | 27.11 | 2.18 | 27.45 | 2.10 | 0.4409 |
| Dental relationships | |||||||
| Overjet (mm) | 6.24A | 2.21 | 8.69B | 2.50 | 4.70C | 1.60 | 0.0000 |
| Overbite (mm) | 4.94 | 1.68 | 4.44 | 2.24 | 4.62 | 1.71 | 0.6434 |
| Molar relationship (mm) | −1.38A | 1.15 | −2.08A | 1.18 | 0.69B | 1.23 | 0.0000 |
Both appliances showed significant and similar restriction of maxillary forward displacement compared with the control group ( Table VII ). Mandibular forward displacement was significantly less in the activator-headgear group. There were significantly greater reductions in the maxillomandibular Class II relationship and facial convexity in both experimental groups than in the control group. The Frankfort-mandibular plane angle and lower anterior face height had significantly greater increases in the experimental groups than in the control groups. The maxillary incisors had significantly greater palatal inclination in the headgear-activator group and significantly greater retrusion and extrusion in the experimental groups. The maxillary molars had significantly greater distalization in the experimental than in the control group, and the headgear-activator group had greater extrusion of these teeth than did the Jasper jumper group. The mandibular incisors had significantly greater labial tipping in the activator-headgear group than in the control group, but significantly greater protrusion and extrusion in the Jasper jumper group than in the control group. The mandibular molars had significantly greater mesialization in the Jasper jumper group than in the other groups, but significantly greater intrusion in the experimental groups. Overjet, overbite, and molar relationships had significantly greater improvements in the experimental groups.


