Fig. 6.1
Dental caries levels (decayed, missing, and filled teeth (DMFT) index) among 12-year-olds worldwide (Reproduced, with the permission of the publisher, from Bulletin of the World Health Organization, Petersen et al. [7]. http://www.who.int/bulletin/volumes/83/9/petersen0905abstract/en/)
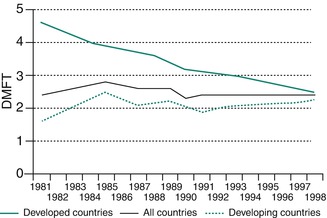
Fig. 6.2
Changing levels of dental caries experience (decayed, missing, and filled teeth (DMFT) index) among 12-year-olds in developed and developing countries (Reproduced, with the permission of the publisher, from Bulletin of the World Health Organization, Petersen et al. [7]. http://www.who.int/bulletin/volumes/83/9/petersen0905abstract/en/)
However, the industrialized countries tell a different story. A steady decline of caries experience is found. This result from a number of public health measures including effective use of fluorides, together with changing living conditions, lifestyles, and improved self-care practices.
Worldwide, the prevalence of dental caries among adults is high as the disease affects nearly 100 % of the population in the majority of countries. Figure 6.3 illustrates the levels of dental caries among 35–44-year-olds, as measured by the mean DMFT index. Most industrialized countries and some countries of Latin America show high DMFT values.
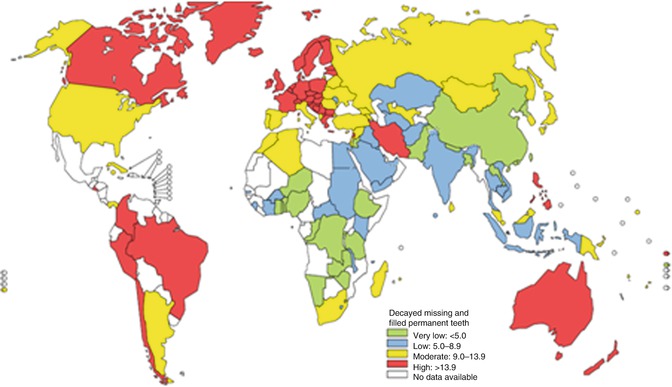
Fig. 6.3
Dental caries levels (decayed, missing, and filled teeth (DMFT) index) among 35–44-year-olds worldwide (Reproduced, with the permission of the publisher, from Bulletin of the World Health Organization, Petersen et al. [7]. http://www.who.int/bulletin/volumes/83/9/petersen0905abstract/en/)
6.1.3 Developing Global Policies Highlighting the Importance of Oral Health
The policy of the WHO Global Oral Health Programme emphasizes that oral health is integral and essential to general health and that oral health is a determinant factor for quality of life. The WHO Global Oral Health Programme has implied that greater emphasis is put on developing global policies based on common risk factors and approaches should be coordinated more effectively with other programs in public health [8–10]:
-
To adopt measures to ensure that oral health is incorporated as appropriate into policies for the integrated prevention and treatment of chronic noncommunicable and communicable diseases and into maternal and child health policies
-
To take measures to ensure that evidence-based approaches are used to incorporate oral health into national policies as appropriate for integrated prevention and control of noncommunicable diseases
-
To consider mechanisms to provide coverage of the population with essential oral health care, to incorporate oral health in the framework of enhanced primary health care for chronic noncommunicable diseases, and to promote the availability of oral health services that should be directed toward disease prevention and health promotion for poor and disadvantaged populations, in collaboration with integrated programs for the prevention of chronic noncommunicable diseases
-
For those countries without access to optimal levels of fluoride, and which have not yet established systematic fluoridation programs, to consider the development and implementation of fluoridation programs, giving priority to equitable strategies such as the automatic administration of fluoride, for example, in drinking water, salt, or milk, and to provide affordable fluoride toothpaste
-
To develop and implement the promotion of oral health and prevention of oral disease for preschool and school children as part of activities in health-promoting schools
-
To scale up capacity to produce oral health personnel, including dental hygienists, nurses, and auxiliaries, providing for equitable distribution of these auxiliaries to the primary-care level and ensuring proper service back-up by dentists through appropriate referral systems
-
To incorporate an oral health information system into health surveillance plans so that oral health objectives are in keeping with international standards and to evaluate progress in promoting oral health
-
To strengthen oral health research and use evidence-based oral health promotion and disease prevention in order to consolidate and adapt oral health programs and to encourage the intercountry exchange of reliable knowledge and experience of community oral health programs
-
To address human resources and workforce planning for oral health as part of every national plan for health
-
To increase, as appropriate, the budgetary provisions dedicated to the prevention and control of oral and craniofacial diseases and conditions
-
To strengthen partnerships and shared responsibility among stakeholders in order to maximize resources in support of national oral health programs
6.2 Caries Burden in China
6.2.1 The First and Second National Epidemiological Investigation of Oral Health in China
China has organized two nationwide epidemiology investigations. The first was conducted between 1982 and 1984, which had examined the status of caries and periodontal diseases in primary and middle school students of 29 provinces, autonomous administration regions, and municipalities directly under the central government. There were altogether 131,340 students examined. The first national epidemiological investigation of oral health in China is the first large-scale epidemiological investigation organized since the establishment of P.R. China.
The second national epidemiological investigation of oral health in China took place from 1995 to 1998. This investigation had included 6 age groups covering 5–74-year-olds from 11 provinces, autonomous administration regions, and municipalities directly under the central government. A total of 140,712 people at 396 sample sites were selected.
Results of these two epidemiology investigations have provided valuable first-hand data for the central government to make oral health-related policies, set up targets for oral health service, and planned future human resource allocation in oral health service.
According to the second national survey which was conducted in 1995, caries prevalence rates for 5-year-olds, 12-year-olds, 35–44-year-olds, and 65–74-year-olds were 76.6 %, 45.8 %, 63.0 %, and 64.8 %, respectively.
6.2.2 The Third National Epidemiological Investigation of Oral Health in China
The third national epidemiological investigation of oral health in China was implemented in 2005. At the planning period, the sampling methods have been carefully designed as stratified multilevel randomized sampling [11]. A total of 93,826 people were selected covering 5–74-year-olds in 6 age groups. The sample well represents the overall status of oral health in China. In addition to dental examinations, a comprehensive questionnaire investigation was simultaneously conducted to investigate the oral health-related concepts and behaviors of the selected sample.
Caries status obtained from stratified populations is detailed as follows.
6.2.2.1 Caries Status of 5-Year-Olds
The 5-year-olds have a caries prevalence rate of 66.0 % in the primary dentition. Children who live in the cities have a slightly lower caries prevalence rate (62.0 %), while in the rural areas, children have a higher caries prevalence rate (70.2 %).
Average DMFT of the 5-year-olds is 3.5, while most of these children have a DMFT of 2, accounting for 11.1 % of the total subsample. The constitution of DMFT indices can be viewed in Fig. 6.4, which has shown that an astonishing proportion of carious teeth have never been treated (96.7 %). Analysis of the frequency distribution of DMFT in children has aroused our attention when it is found that 79.3 % of all carious teeth concentrate in about one-third of the examined children, who present a significant caries index of 8.33.
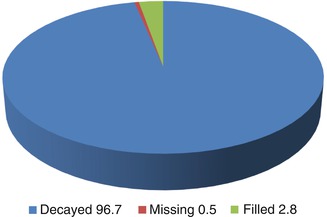
Fig. 6.4
Constitution of decayed, missing, and filled teeth in 5-year-olds in China (%)
Approximately half of the subsample have their guardians (mostly parents and grandparents) completed the questionnaire. It has been found that 13 % children began to brush their teeth before the age of 3, and the remaining vast majority has just begun to brush their teeth. Around one-fifth of children don’t brush their teeth.
There were 49 % parents aware of the fluoride toothpaste, and 39 % of 5-year-olds use the fluoridated toothpaste when brushing their teeth. It should be paid attention to that only 22 % children visit dentists periodically. The most common reasons for dental visits are acute or chronic toothache and other reasons such as dental emergency.
Multiple regression analysis was performed to examine the main reasons for caries in children. It has been found that urban/rural distribution, sugar consumption before sleeping, toothbrushing starting age, and oral hygiene by parents all correlate with caries status of children.
6.2.2.2 Caries Status of 12-Year-Olds
Caries prevalence rate of the 12-year-olds is 28.9 %. No difference is observed between urban and rural areas, and boys have a statistically significant lower caries prevalence rate than girls (25.4 % vs. 32.6 %).
The most often affected teeth are mandibular first molars, maxillary first molars, and mandibular second molars. Unfortunately, 88.8 % of all carious teeth have not been treated (Fig. 6.5). In China, 1.45 % of 12-year-olds have pit and fissure sealants, and there is a huge difference between urban area and rural area (2.75 % vs. 0.19 %).
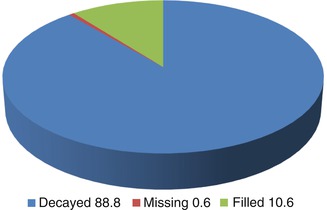
Fig. 6.5
Constitution of decayed, missing, and filled teeth in 12-year-olds in China (%)
The investigated 12-year-olds have completed the questionnaire by themselves. As this age group is the most important age group, it has been receiving continuous attention from the central government. In addition to questions on oral health-related knowledge and behavior, the questionnaire has also included questions on dental visits and self-perceived impact of oral health.
It has been found that 82 % of the 12-year-olds investigated brush their teeth daily; however, only 28 % of them brush their teeth at least twice a day. Ninety-three percent of the children report that they have never used dental floss. The percentage of children who use fluoridated toothpaste is 46 %. Sixty-nine percent of the children have daily consumption of sugar-containing food, such as sweetened milk, dissert, candy, carbonated soft drink, and sweetened fruit juice. It is satisfactory that only a small fraction of the investigated children smoke (boys 5.7 % and girls 0.5 %) and that the percentage of daily consumption of cigarette and alcohol is further reduced to 1.0 % and 0.1 %, respectively, for boys and girls.
With regard to oral health-related knowledge, only one-tenth of 12-year-olds understand dental plaque as the cause for caries and periodontal diseases. However, over 60 % of them have realized that bleeding during toothbrushing is abnormal.
In the past 12 months, 21 % of 12-year-olds have visited a dentist. However, 47 % of the total subsample have never seen a dentist. The most common reasons for their dental visit are acute or chronic toothache. It is sad that only 28 % have formed the habit of frequent dental check-ups.
6.2.2.3 Caries Status of 35–44-Year-Olds
The 35–44-year-olds is the WHO recommended age group for adults. It has been found that the vast majority of this age group (88.1 %), quite unfortunately, has been affected by caries. Not much difference was found between the urban and rural populations (89.1 % vs. 87.1 %). However, women are found with statistically significant higher caries prevalence rate than men (91.3 % vs. 84.9 %). The constitution of the DMFT indices is shown in Fig. 6.6. However, the prevalence rate for root caries is near one-third (32.7 %), signifying bad periodontal status.
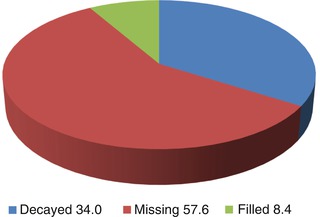
Fig. 6.6
Constitution of decayed, missing, and filled teeth in 35–44-year-olds in China (%)
All of the investigated subgroup answered the questionnaire. Among all the 35–44-year-olds, 89 % have reported that they brush their teeth daily, and 35 % have reported to be brushing their teeth at least twice a day. Better teeth brushing habits are found in cities, women than in rural areas and men.
On a daily basis, 27 % use toothpicks, but over 99 % do not use dental floss. Fluoridated toothpaste is used in 46 % people. Daily consumption of sugar is found in 21 % of those investigated. There are 32 % questionnaire respondents reported to be smokers. There is a huge gender difference in daily alcohol consumption, while 23 % men, in contrast to 2 % women, drink alcohol daily.
Among the 35–44-year-olds, 69 % believe there is a need for them to receive oral treatment, and the percentage is found to be statistically significantly higher in urban populations than rural (73 % vs. 65 %). However, in the past 12 months, only 16 % of them have been to a dentist. Quite surprisingly, even at this age, there are as many as 46 % 35–44-year-olds who have never visited a dentist ever. For the remaining 54 %, the majority of them have attributed their dental attendance to be because of acute or chronic toothache or other dental situations, and few of them have formed the habit of regular dental check-ups.
Multiple regression analysis has revealed that the caries status of the 35–44-year-olds is closely related to the use of fluoride toothpaste, consumption of sugar-containing foods, toothbrushing frequencies, and other behavioral variables. Those with no use of fluoridated toothpaste, with daily consumption of sugar-containing foods, and who are not brushing their teeth on a daily basis manifest with high caries risk.
6.2.2.4 Caries Status of 65–74-Year-Olds
Caries prevalence in the age group of 65–74-year-olds is found to be very high. The prevalence rate is as high as 98.4 %, and not much difference is found between urban and rural populations. Also, not much difference is discovered between both genders. The mean DMFT score is 14.7, the majority of which is missing due to caries (75.3 %), and only a fraction of the iceberg is treated (1.9 %) (Fig. 6.7).
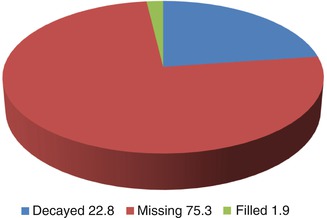
Fig. 6.7
Constitution of decayed, missing, and filled teeth in 65–74-year-olds in China (%)
Root caries is another important issue that should not be neglected. The age group of 65–74-year-olds are found to be heavily affected by caries in the root. Rural population have a root caries prevalence rate of 67.2 %, higher than the urban population (60.0 %). It is found that 66.1 % females are affected by root caries, higher than males (61.1 %). It is further discovered that only as low as 1.9 % of all the carious lesions in the root have been treated (Fig. 6.8).
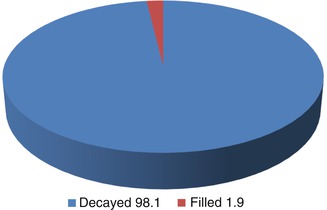
Fig. 6.8
Constitution of decayed and filled root caries in 65–74-year-olds in China (%)
About half of the examined subjects have handed in the questionnaire. It has been found that three-quarters of the questionnaire respondents brush their teeth on a daily basis and that slightly over one-quarter brush their teeth twice a day. This self-oral hygiene behavior is found to be better in cities and females. In 27 % of the questionnaire respondents, fluoridated toothpaste is used; the percentage is found to be higher in cities than in rural areas. There are 26 % of the respondents who report they use toothpick daily, but almost none of the respondents have ever used dental floss.
Daily sugar-containing food consumption is found in 27 % questionnaire respondents. An average of 27 % of the respondent smoke, and there is a huge difference between the two genders. And it is found that among those who smoke, 90 % of them have been smoking for more than 20 years. Alcohol consumption is found in 13.6 % respondents; the percentage of male is almost six times that of the female.
Over half of the elder population believe they are in need of oral examination and treatment; however, only 19 % of the respondents report that they have visited a dentist within the past 12 months. The most common reason for dental referral is acute and chronic toothache. However, it is unfortunate that about one-third of the all the respondents have never been to a dentist for any form of oral examination or treatment. For the expenditure on dental visits, 83 % of the respondents report that they are fully self-financed, not to be able to find a source to partly cover the bill.
When we analyze the oral health impact on daily life, it is sad to find that over half the respondents have experienced toothache, and the majority of the elders are not satisfied with their oral hygiene conditions.
6.3 Caries Preventive Strategies
Dental caries results from a variety of contributing factors. There are three most important factors, namely, cariogenic microflora (termed as dental plaque), carbohydrate-rich diet, and susceptible teeth. Given time, the interrelation and interaction between these three factors will produce the chronic oral disease which brings pain and discomfort to the majority of the population worldwide since an early age. Therefore, effective caries-preventive strategies almost always require removal of any or all of these contributing factors.
There is a hierarchy of caries-preventive strategies which include the following.
6.3.1 Primary Prevention
Primary prevention is the most important strategy as it stresses and deals with combating the etiological factors. Self-awareness with regard to caries prevention is often highlighted in this stage. People are motivated by a variety of means, either with propaganda via mass media or face-to-face educational lectures, so that they will be self-conscious about the importance of keeping good oral hygiene, restricting the consumption of sugars and frequent dental visits.
Many countries have set up their own launches or campaigns to deliver the concept of oral health education. China, for example, has launched its own national campaign for over a decade. Each year on the “love teeth day” on September 20th, there will be dental health educational and promotional activities held across the country. There is a unique theme every year. Usually manuals containing educational information are distributed free of charge. In many cities where there are dental schools or colleges, free dental check-ups are available.
Removal of etiological factors is very important in this stage. The main methods include dental plaque control, use of fluoride, and other preventive methods that are to be introduced in the following section.
6.3.2 Secondary Prevention
Secondary prevention mainly refers to the early diagnosis and treatment of lesions found to be still at their early stages. For a long time, caries diagnosis mainly relies heavily on the dentists themselves who can only resort to their naked eyes and self-practicing experiences. This has resulted in countless mistaken diagnosis and omission of countless lesions which had been left not dealt with. Later, the invention of X-ray has offered another possibility to visualize lesions that hide from usual visual examination.
6.3.2.1 Conventional Caries Detection Methods
Traditional diagnostic methods, such as visual inspection, appear to have very low sensitivity and high specificity in diagnosing caries [12–14]. Continuous attempts to improve the sensitivity have been made. Ekstrand et al have proposed a new caries scoring system as presented in Table 6.1. Sensitivity and specificity for detection of dentinal lesions were found to be ranging between 0.92 and 0.97 and 0.85 and 0.93, respectively [15
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


