The iliac crest has been used for graft reconstruction of the maxillofacial region for many decades. It was not until 1979 that a reliable vascular supply to the anterior ilium was elucidated by Taylor and co-workers, and this flap was routinely used for microvascular free tissue transfer. It has since been applied to reconstruction of the mandible and maxilla and used as a composite flap for complex defects of the face. The vascular anatomy is reliable, and success rates are high.
Anatomy
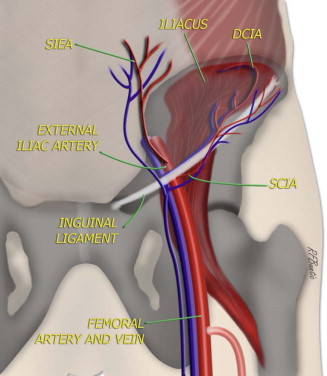
The deep circumflex iliac artery (DCIA) ( Fig. 72-1 ) originates from the lateral portion of the external iliac artery just above the inguinal ligament. It is a robust artery that is generally 2 to 3 mm in diameter. The DCIA ascends parallel to the inguinal ligament to a point medial to the anterior superior iliac spine (ASIS) and then penetrates the transversalis fascia and continues its course along the medial lip of the iliac crest between the iliacus and transversus abdominis muscles. The main course of the artery serves the bone of the iliac crest through periosteal and endosteal branches. The bone supplied extends from the ASIS to the sacroiliac joint. Perforating vessels to the surrounding soft tissues are somewhat variable. In the majority of patients (70% to 80%), a large (1 mm) single vessel termed the ascending branch originates from the DCIA and serves the internal oblique muscle. A minority of individuals have multiple perforating vessels serving the muscular layers of the abdominal wall rather than a well-defined ascending branch. On rare occasions (1%), the ascending branch will directly join the external iliac artery. In these situations, if one desires to use the internal oblique muscle as part of the reconstruction, a separate anastomosis of this vessel will also need to be performed, as well as the DCIA. Perforating vessels to the skin arise 6 to 9 cm posterior to the ASIS and 2 to 3 cm medial to the crest. One dominant perforator or several smaller ones are required for reliable vascular supply to the skin. These skin perforators arise from branches that perforate all three muscular layers of the abdominal wall (transversus abdominis, internal oblique, and external oblique).
Venous drainage of the flap generally follows the arterial anatomy. Accompanying the smaller arteries are paired venae comitantes. These vessels usually combine to form a single deep circumflex iliac vein several centimeters above the external iliac vein, which provides a 3- to 5-mm vein for venous anastomosis. Occasionally, the venae comitantes will not join, thus making two venous anastomoses advisable.
The motor nerves to the muscles of the abdominal wall are segmental and arise from the lower thoracic and upper lumbar levels. They are not generally suitable for providing dynamic muscular reinnervation to a flap. The lateral femoral cutaneous nerve provides sensation to the lateral thigh skin. It courses in the fascia above the iliacus muscle medial to the ASIS. Its course relative to the DCIA is variable. When it is deep to the vascular pedicle, it can usually be preserved without much difficulty. Occasionally, it will be found superficial to the vessels and requires division. Patients should be informed preoperatively about the resulting sensory disturbance. The surgeon should be aware that the femoral nerve runs with the external iliac artery and vein as they pass under the inguinal ligament. Although it will not generally be visualized during dissection, placement of sutures in this area during closure could potentially place it at risk.
The muscular anatomy in this area is primarily related to the layers of the abdominal wall. In addition, the iliacus muscle runs along the medial aspect of the ilium. The flexors of the hip attach along the lateral ilium and the sartorius tendon to the ASIS.
Diagnostic Studies
The iliac artery is prone to atherosclerotic changes, but the DCIA is relatively immune. Therefore, preoperative vascular imaging studies are not usually recommended. Preoperative pencil Doppler ultrasonography is used to locate perforating vessels to the skin medial to the iliac crest when a skin paddle is required for composite reconstruction. Previous surgeries such as appendectomy and repair of an inguinal hernia can affect the vascular anatomy and should be taken into consideration when present. An alternative flap should be selected for patients who have previously undergone vascular bypass surgery in the inguinal region.
Diagnostic Studies
The iliac artery is prone to atherosclerotic changes, but the DCIA is relatively immune. Therefore, preoperative vascular imaging studies are not usually recommended. Preoperative pencil Doppler ultrasonography is used to locate perforating vessels to the skin medial to the iliac crest when a skin paddle is required for composite reconstruction. Previous surgeries such as appendectomy and repair of an inguinal hernia can affect the vascular anatomy and should be taken into consideration when present. An alternative flap should be selected for patients who have previously undergone vascular bypass surgery in the inguinal region.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


